

Three-dimensional ultrashort echo time magnetic resonance imaging in assessment of idiopathic pulmonary fibrosis, in comparison with high-resolution computed tomography
- PMID: 35919053
- PMCID: PMC9338383
- DOI: 10.21037/qims-21-1133
Three-dimensional ultrashort echo time magnetic resonance imaging in assessment of idiopathic pulmonary fibrosis, in comparison with high-resolution computed tomography
Abstract
Background: We aimed to evaluate the image quality, feasibility, and diagnostic performance of three-dimensional ultrashort echo time magnetic resonance imaging (3D UTE-MRI) to assess idiopathic pulmonary fibrosis (IPF) compared with high-resolution computed tomography (HRCT) and half-Fourier single-shot turbo spin-echo (HASTE) MRI.
Methods: A total of 36 patients with IPF (34 men; mean age: 62±8 years, age range: 43 to 78 years) were prospectively included and underwent HRCT and chest MRI on the same day. Chest MRI was performed with a free-breathing 3D spiral UTE pulse sequence and HASTE sequence on a 1.5 T MRI. Two radiologists independently evaluated the image quality of the HRCT, HASTE, and 3D UTE-MRI. They assessed the representative imaging features of IPF, including honeycombing, reticulation, traction bronchiectasis, and ground-glass opacities. Image quality of the 3D UTE-MRI, HASTE, and HRCT were assessed using a 5-point visual scoring method. Kappa and weighted kappa analysis were used to measure intra- and inter-observer and inter-method agreements. Sensitivity (SE), specificity (SP), and accuracy (AC) were used to assess the performance of 3D UTE-MRI for detecting image features of IPF and monitoring the extent of pulmonary fibrosis. Linear regressions and Bland-Altman plots were generated to assess the correlation and agreement between the assessment of the extent of pulmonary fibrosis made by the 2 observers.
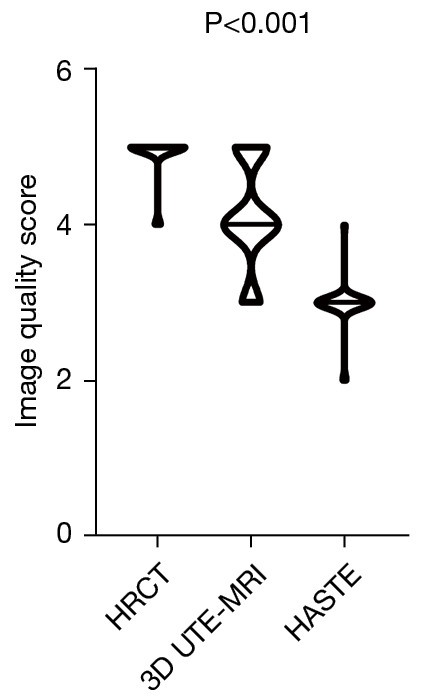
Results: The image quality of HRCT was higher than that of HASTE and UTE-MRI (HRCT vs. UTE-MRI vs. HASTE: 4.9±0.3 vs. 4.1±0.7 vs. 3.0±0.3; P<0.001). Interobserver agreement of HRCT, HASTE, and 3D UTE-MRI when assessing pulmonary fibrosis was substantial and excellent (HRCT: 0.727≤ κ ≤1, P<0.001; HASTE: 0.654≤ κ ≤1, P<0.001; 3D UTE-MRI: 0.719≤ κ ≤0.824, P<0.001). In addition, reticulation (SE: 97.1%; SP: 100%; AC: 97.2%; κ =0.654), honeycombing (SE: 83.3%; SP: 100%; AC: 86.1%; κ =0.625) patterns, and traction bronchiectasis (SE: 94.1%; SP: 100%; AC: 94.4%, κ =0.640) were also well-visualized on 3D UTE-MRI, which was significantly superior to HASTE. Compared with HRCT, the sensitivity of 3D UTE-MRI to detect signs of pulmonary fibrosis (n=35) was 97.2%. The interobserver agreement in elevation of the extent of pulmonary fibrosis with HRCT and 3D UTE-MRI was R2=0.84 (P<0.001) and R2=0.84 (P<0.001), respectively. The extent of pulmonary fibrosis assessed with 3D UTE-MRI [median =9, interquartile range (IQR): 6.25 to 10.00] was lower than that from HRCT (median =12, IQR: 9.25 to 13.00; U=320.00, P<0.001); however, they had a positive correlation (R=0.72, P<0.001).
Conclusions: As a radiation-free non-contrast enhanced imaging method, although the image quality of 3D UTE-MRI is inferior to that of HRCT, it has high reproducibility to identify the imaging features of IPF and evaluate the extent of pulmonary fibrosis.
Keywords: Lungs; high-resolution computed tomography (HRCT); idiopathic pulmonary fibrosis (IPF); three-dimensional ultrashort echo time magnetic resonance imaging (3D UTE-MRI).
2022 Quantitative Imaging in Medicine and Surgery. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://qims.amegroups.com/article/view/10.21037/qims-21-1133/coif). TB is employed by Siemens Healthcare GmbH and JA is employed by Siemens Shenzhen Magnetic Resonance Ltd. The other authors have no conflicts of interest to declare.
Figures






References
-
- Puderbach M, Eichinger M, Haeselbarth J, Ley S, Kopp-Schneider A, Tuengerthal S, Schmaehl A, Fink C, Plathow C, Wiebel M, Demirakca S, Müller FM, Kauczor HU. Assessment of morphological MRI for pulmonary changes in cystic fibrosis (CF) patients: comparison to thin-section CT and chest x-ray. Invest Radiol 2007;42:715-25. 10.1097/RLI.0b013e318074fd81 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials