

Impact of a Laboratory-Developed Phenotypic Rapid Susceptibility Test Directly From Positive Blood Cultures on Time to Narrowest Effective Therapy in Patients With Gram-Negative Bacteremia: A Prospective Randomized Trial
- PMID: 35919072
- PMCID: PMC9339149
- DOI: 10.1093/ofid/ofac347
Impact of a Laboratory-Developed Phenotypic Rapid Susceptibility Test Directly From Positive Blood Cultures on Time to Narrowest Effective Therapy in Patients With Gram-Negative Bacteremia: A Prospective Randomized Trial
Abstract
Background: Antimicrobial susceptibility testing (AST) is often needed prior to antimicrobial optimization for patients with gram-negative bloodstream infections (GN-BSIs). Rapid AST (rAST) in combination with antimicrobial stewardship (AS) may decrease time to administration of narrower antibiotics.
Methods: This was a prospective, nonblinded, randomized trial evaluating the impact of a phenotypic rAST method vs conventional AST (cAST) in hospitalized patients with GN-BSI and source control. The primary outcome was time to narrowest effective therapy.
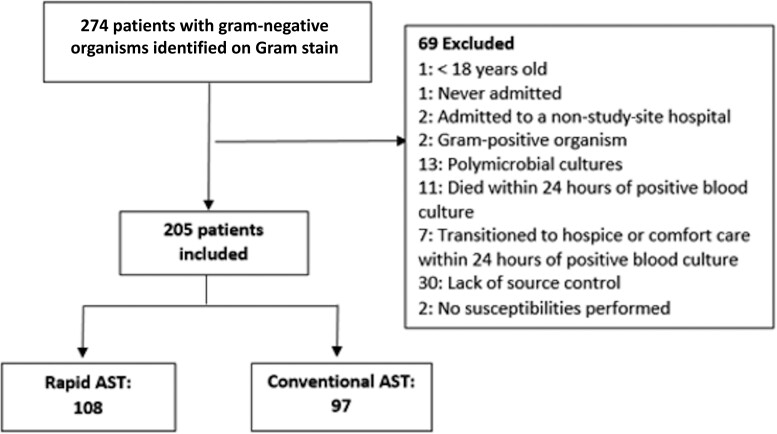
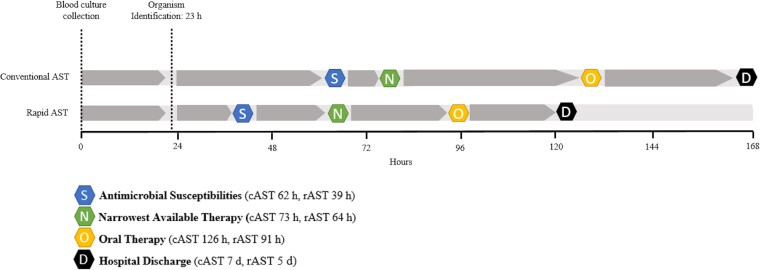
Results: Two hundred seventy-four patients were randomized and 205 underwent analysis (97 cAST, 108 rAST). Median (interquartile range [IQR]) time to susceptibility results was 23 hours shorter in the rAST group (cAST: 62 [59-67] hours vs rAST: 39 [IQR, 35-46] hours; P < .001). Median (IQR) time to narrowest effective therapy was similar between groups (cAST: 73 [44-138] hours vs rAST: 64 [42-92] hours; P = .10). Median (IQR) time to narrowest effective therapy was significantly shorter in a prespecified subgroup of patients not initially on narrowest therapy and during AS working hours (cAST: 93 [56-154] hours vs rAST: 62 [43-164] hours; P = .004). Significant decreases were observed in median (IQR) time to oral therapy (cAST: 126 [76-209] hours vs rAST: 91 [66-154] hours; P = .02) and median (IQR) length of hospital stay (cAST: 7 [4-13] days vs rAST: 5 [4-8] days; P = .04).
Conclusions: In patients with GN-BSI, rAST did not significantly decrease time to narrowest effective therapy but did decrease time to oral antibiotics and length of hospital stay. Rapid AST using existing microbiology platforms has potential to optimize patient outcomes.
Keywords: antimicrobial stewardship; antimicrobial susceptibility testing; bloodstream infection; gram negative; rapid diagnostic testing.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
Similar articles
-
Randomized Trial Evaluating Clinical Impact of RAPid IDentification and Susceptibility Testing for Gram-negative Bacteremia: RAPIDS-GN.Clin Infect Dis. 2021 Jul 1;73(1):e39-e46. doi: 10.1093/cid/ciaa528. Clin Infect Dis. 2021. PMID: 32374822 Free PMC article. Clinical Trial.
-
Rapid determination of antimicrobial susceptibility of Gram-negative bacteria from clinical blood cultures using a scattered light-integrated collection device.J Med Microbiol. 2024 Feb;73(2). doi: 10.1099/jmm.0.001812. J Med Microbiol. 2024. PMID: 38415707
-
Impact of EUCAST rapid antimicrobial susceptibility testing (RAST) on management of Gram-negative bloodstream infection.Infect Dis Now. 2022 Nov;52(8):421-425. doi: 10.1016/j.idnow.2022.09.002. Epub 2022 Sep 13. Infect Dis Now. 2022. PMID: 36108973
-
Rapid microbiological tests for bloodstream infections due to multidrug resistant Gram-negative bacteria: therapeutic implications.Clin Microbiol Infect. 2020 Jun;26(6):713-722. doi: 10.1016/j.cmi.2019.09.023. Epub 2019 Oct 11. Clin Microbiol Infect. 2020. PMID: 31610299 Review.
-
How to accelerate antimicrobial susceptibility testing.Clin Microbiol Infect. 2019 Nov;25(11):1347-1355. doi: 10.1016/j.cmi.2019.04.025. Epub 2019 May 2. Clin Microbiol Infect. 2019. PMID: 31055166 Review.
Cited by
-
Management of Bacterial and Fungal Infections in the ICU: Diagnosis, Treatment, and Prevention Recommendations.Infect Drug Resist. 2023 May 4;16:2709-2726. doi: 10.2147/IDR.S390946. eCollection 2023. Infect Drug Resist. 2023. PMID: 37168515 Free PMC article. Review.
-
Evaluating the impact of rapid antimicrobial susceptibility testing for bloodstream infections: a review of actionability, antibiotic use and patient outcome metrics.J Antimicrob Chemother. 2024 Sep 19;79(12 Suppl 2):i13-i25. doi: 10.1093/jac/dkae282. J Antimicrob Chemother. 2024. PMID: 39298359 Free PMC article. Review.
-
Performance of the Vitek 2 Advanced Expert System (AES) as a Rapid Tool for Reporting Antimicrobial Susceptibility Testing (AST) in Enterobacterales from North and Latin America.Microbiol Spectr. 2023 Feb 14;11(1):e0467322. doi: 10.1128/spectrum.04673-22. Epub 2023 Jan 16. Microbiol Spectr. 2023. PMID: 36645286 Free PMC article.
-
The Impact of Reporting the Same-Day Identification and Antibiotic Susceptibility Test Results on the Treatment of Bloodstream Infections.Infect Dis Clin Microbiol. 2024 Jun 28;6(2):123-132. doi: 10.36519/idcm.2024.334. eCollection 2024 Jun. Infect Dis Clin Microbiol. 2024. PMID: 39005703 Free PMC article.
-
Delving into discrepancies, a single-center experience with Accelerate Pheno for gram-negative bacteremia, a rapid phenotypic susceptibility testing method.Antimicrob Steward Healthc Epidemiol. 2025 Jan 23;5(1):e15. doi: 10.1017/ash.2024.482. eCollection 2025. Antimicrob Steward Healthc Epidemiol. 2025. PMID: 39911512 Free PMC article.
References
-
- Kang C-I, Kim S-H, Park WB, et al. . Bloodstream infections caused by antibiotic-resistant gram-negative bacilli: risk factors for mortality and impact of inappropriate initial antimicrobial therapy on outcome. Antimicrob Agents Chemother 2005; 49:760–6. doi:10.1128/AAC.49.2.760-766.2005 - DOI - PMC - PubMed
-
- Lodise TP, Kanakamedala H, Hsu WC, Cai B. Impact of incremental delays in appropriate therapy on the outcomes of hospitalized adult patients with gram-negative bloodstream infections: “Every day matters.” Pharmacotherapy 2020; 40:889–901. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
