

Neuromyelitis optica spectrum disorders and anti-myelin oligodendrocyte glycoprotein positive optic neuropathies
- PMID: 35919317
- PMCID: PMC9318083
- DOI: 10.18240/ijo.2022.07.09
Neuromyelitis optica spectrum disorders and anti-myelin oligodendrocyte glycoprotein positive optic neuropathies
Abstract
Aim: To describe the clinical characteristics and treatments associated with antibody positive optic neuropathies including anti-myelin oligodendrocyte glycoprotein (MOG) and anti-aquaporin 4 (AQP4), alongside diagnostic modalities, investigations, and outcomes.
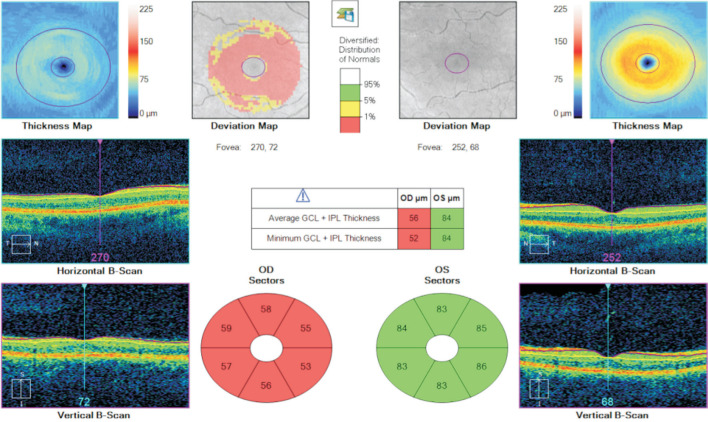
Methods: A cross-sectional single-centre retrospective case series consisting of 16 patients including 12 anti-MOG positive patients and 4 anti-AQP4 positive patients. Each of these patients had clinical signs and symptoms of optic neuritis and consisted of all patients who had a positive blood antibody result in our centre. Clinical findings including presence of a relative afferent pupillary defect, colour vision and disc assessment were recorded. Structured clinical exam and multimodal imaging was undertaken sequentially on each. Optical coherence tomography (OCT) scanning was preformed to examine the correlation between ganglion cell layer (GCL) thickness and visual acuity (VA) at presentation and as a determinant of final visual outcome in both groups. Initial and long-term treatment is also summarised.
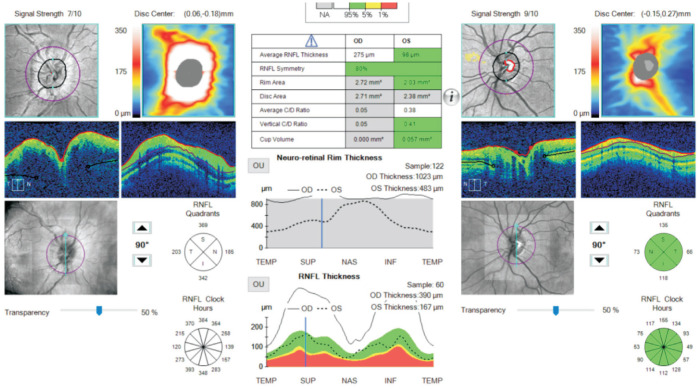
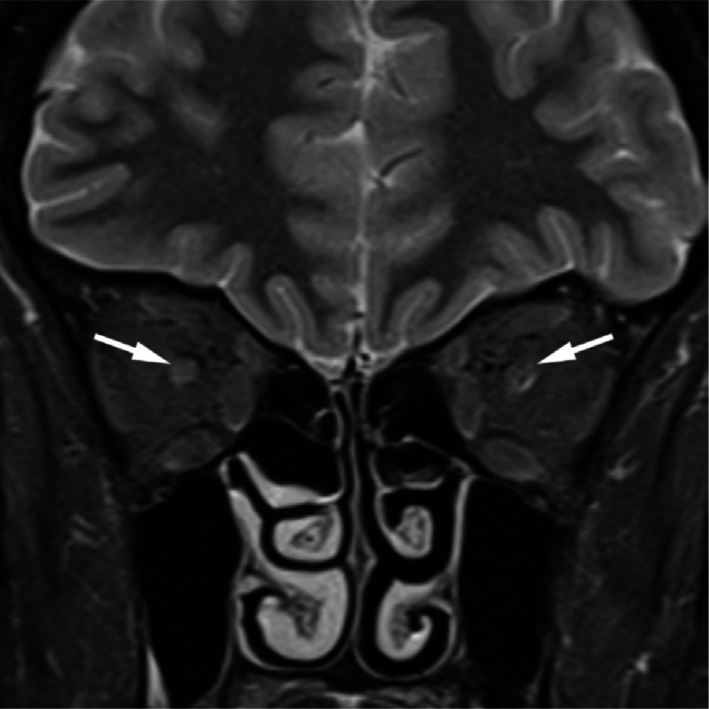
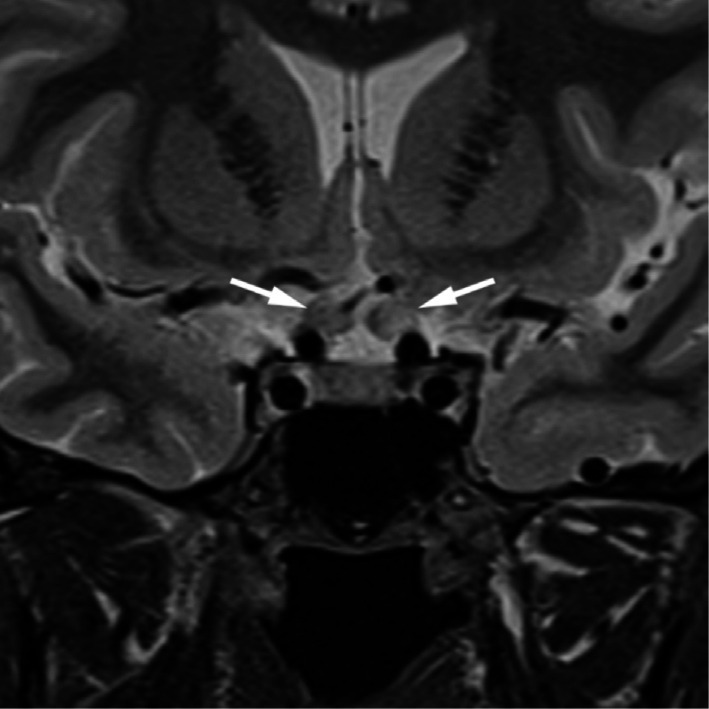
Results: A total of 16 patients were included in the study consisting of 12 anti-MOG and 4 anti-AQP4 positive patients. Nine of the 16 patients were female and the average age of onset was 29.2y in the MOG group and 42y in the AQP4 group. There was no statistically significant correlation (Pearson correlation) between GCL thickness and presenting and final VA [r(10)=0.081, P=0.08 and r(10)=0.089, P=0.34 respectively]. The same statistical analysis was performed for the correlation between retinal nerve fibre layer (RNFL) and VA and similar outcomes were observed [r(10)=0.04, P=0.22 and r(10)=0.09, P=0.04]. No correlation was seen for initial RNFL thickness and final visual outcome in this group either [r(2)=0.19, P=0.38]. Visual field testing and radiological findings for each group are described.
Conclusion: No correlation between initial VA or RNFL and final visual outcome is identified. A broad range of visual field and radiographic findings are identified, a consensus on treatment of neuromyelitis optica spectrum disorders and anti-MOG positive optic neuropathies has yet to be accepted but initial high dose immunosuppression followed by low dose maintenance therapy is favoured.
Keywords: anti-aquaporin 4; anti-myelin oligodendrocyte glycoprotein; antibody; neuromyelitis.
International Journal of Ophthalmology Press.
Figures

Similar articles
-
MOG-IgG in NMO and related disorders: a multicenter study of 50 patients. Part 4: Afferent visual system damage after optic neuritis in MOG-IgG-seropositive versus AQP4-IgG-seropositive patients.J Neuroinflammation. 2016 Nov 1;13(1):282. doi: 10.1186/s12974-016-0720-6. J Neuroinflammation. 2016. PMID: 27802824 Free PMC article.
-
Retinal Nerve Fiber Layer May Be Better Preserved in MOG-IgG versus AQP4-IgG Optic Neuritis: A Cohort Study.PLoS One. 2017 Jan 26;12(1):e0170847. doi: 10.1371/journal.pone.0170847. eCollection 2017. PLoS One. 2017. PMID: 28125740 Free PMC article.
-
Clinical characteristics and prognosis of myelin oligodendrocyte glycoprotein antibody-seropositive paediatric optic neuritis in China.Br J Ophthalmol. 2019 Jun;103(6):831-836. doi: 10.1136/bjophthalmol-2018-312399. Epub 2018 Jul 26. Br J Ophthalmol. 2019. PMID: 30049802
-
Optic neuropathies post-Covid 19 - review.Rom J Ophthalmol. 2022 Oct-Dec;66(4):289-298. doi: 10.22336/rjo.2022.54. Rom J Ophthalmol. 2022. PMID: 36589322 Free PMC article. Review.
-
Changes of retinal structure and visual function in patients with demyelinating transverse myelitis.Neurol Sci. 2022 Nov;43(11):6425-6431. doi: 10.1007/s10072-022-06315-1. Epub 2022 Aug 8. Neurol Sci. 2022. PMID: 35939134 Review.
Cited by
-
Acute Optic Neuropathy in Older Adults: Differentiating Between MOGAD Optic Neuritis and Nonarteritic Anterior Ischemic Optic Neuropathy.Neurol Neuroimmunol Neuroinflamm. 2024 May;11(3):e200214. doi: 10.1212/NXI.0000000000200214. Epub 2024 Mar 28. Neurol Neuroimmunol Neuroinflamm. 2024. PMID: 38547435 Free PMC article.
-
Neuroimaging in atypical normal tension glaucoma: debating routine implementation in the absence of classic neurological findings.Int J Ophthalmol. 2024 Mar 18;17(3):509-517. doi: 10.18240/ijo.2024.03.13. eCollection 2024. Int J Ophthalmol. 2024. PMID: 38721514 Free PMC article.
-
MOG antibody-associated optic neuritis.Eye (Lond). 2024 Aug;38(12):2289-2301. doi: 10.1038/s41433-024-03108-y. Epub 2024 May 23. Eye (Lond). 2024. PMID: 38783085 Free PMC article. Review.
-
CD4+CD25+ regulatory T cell therapy in neurological autoimmune diseases.PeerJ. 2025 Jun 12;13:e19450. doi: 10.7717/peerj.19450. eCollection 2025. PeerJ. 2025. PMID: 40525111 Free PMC article. Review.
References
-
- Sato DK, Callegaro D, Lana-Peixoto MA, Waters PJ, de Haidar Jorge FM, Takahashi T, Nakashima I, Apostolos-Pereira SL, Talim N, Simm RF, Lino AMM, Misu T, Leite MI, Aoki M, Fujihara K. Distinction between MOG antibody-positive and AQP4 antibody-positive NMO spectrum disorders. Neurology. 2014;82(6):474–481. - PMC - PubMed
-
- Reindl M, Waters P. Myelin oligodendrocyte glycoprotein antibodies in neurological disease. Nat Rev Neurol. 2019;15(2):89–102. - PubMed
-
- Ma XY, Kermode AG, Hu XQ, Qiu W. NMOSD acute attack: Understanding, treatment, and innovative treatment prospect. J Neuroimmunol. 2020;348:577387. - PubMed
-
- He D, Li Y, Dai QQ, Zhang YF, Xu Z, Li Y, Cai G, Chu L. Myopathy associated with neuromyelitis optica spectrum disorders. Int J Neurosci. 2016;126(10):863–866. - PubMed
LinkOut - more resources
Full Text Sources