

Assessment of the systolic rise time by photoplethysmography in peripheral arterial diseases: a comparative study with ultrasound Doppler
- PMID: 35919340
- PMCID: PMC9242071
- DOI: 10.1093/ehjopen/oeac032
Assessment of the systolic rise time by photoplethysmography in peripheral arterial diseases: a comparative study with ultrasound Doppler
Abstract
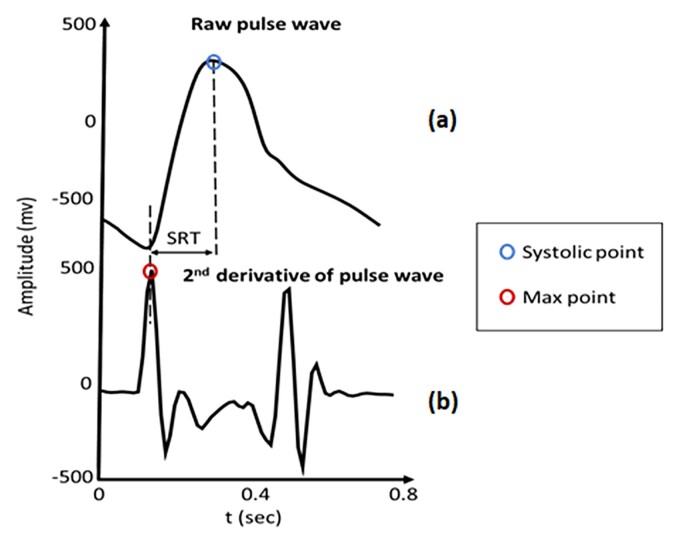
Aims: Peripheral arterial disease (PAD) is a major public health burden requiring more intensive population screening. Ankle brachial index (ABI) using arm and ankle cuffs is considered as the reference method for the detection of PAD. Although it requires a rigorous methodology by trained operators, it remains time-consuming and more technically difficult in patients with diabetes due to mediacalcosis. Techniques based on the study of hemodynamic, such as the systolic rise time (SRT), appear promising but need to be validated. We retrospectively compared the reliability and accuracy of SRT using a photoplethysmography (PPG) technique to the SRT measured by ultrasound doppler (UD) in PAD patients diagnosed with the ABI (137 patients, 200 lower limbs).
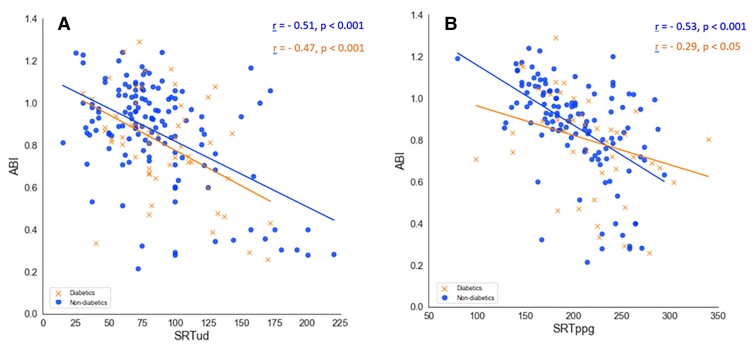
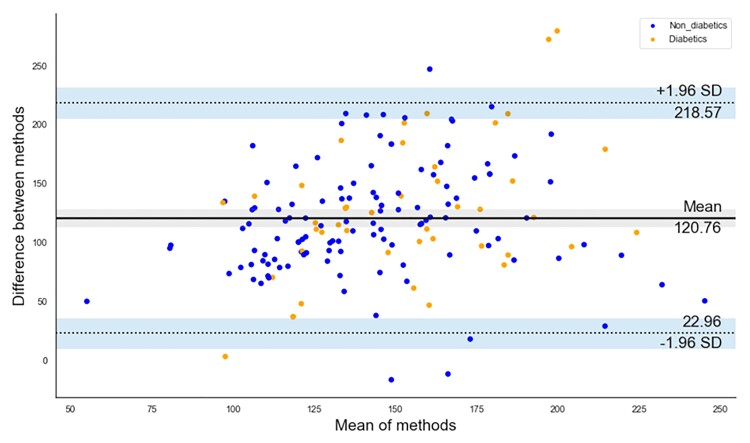
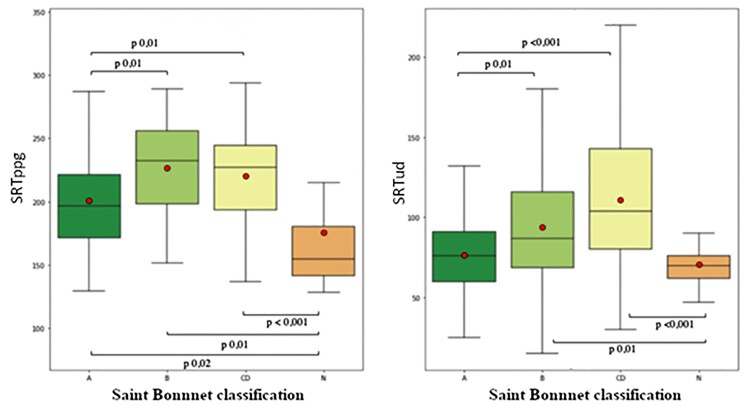
Methods and results: There was a significant correlation between SRT measured with UD (SRTud) compared with that with PPG (SRTppg, r = 0.25; P = 0.001). Best correlation was found in patients without diabetes (r = 0.40; P = 0.001). Bland and Altman analysis showed a good agreement between the SRTud and SRTppg. In contrast, there was no significant correlation between UD and PPG in diabetes patients. Furthermore, patients with diabetes exhibited a significant increase of SRTppg (P = 0.02) compared with patients without diabates but not with the SRTud (P = 0.18). The SRTppg was significantly linked to the arterial velocity waveforms, the type of arterial lesion but not vascular surgery revascularization technique.
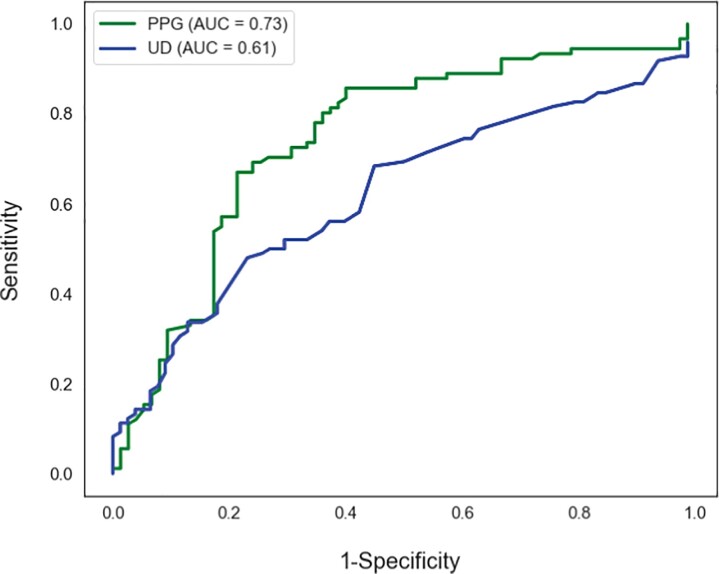
Conclusion: This monocentric pilot study shows that SRT measured with the PPG signal reliably correlates with SRT recorded with UD. The PPG is an easy to use technique in the hand of non-expert with a potential interest for general screening of PAD, especially in diabetes patients, due to its ease to use.
Keywords: Diabetes; Doppler; Peripheral arterial disease; Photoplethysmography.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Figures


Similar articles
-
Photoplethysmography: a simplified method for the office measurement of ankle brachial index in individuals with diabetes.Endocr Pract. 2013 May-Jun;19(3):439-43. doi: 10.4158/EP12172.OR. Endocr Pract. 2013. PMID: 23337138
-
Photoplethysmography and continuous-wave Doppler ultrasound as a complementary test to ankle-brachial index in detection of stenotic peripheral arterial disease.Angiology. 2013 May;64(4):314-20. doi: 10.1177/0003319712464814. Epub 2012 Nov 15. Angiology. 2013. PMID: 23162005
-
Tissue optical perfusion pressure: a simplified, more reliable, and faster assessment of pedal microcirculation in peripheral artery disease.Am J Physiol Heart Circ Physiol. 2020 Dec 1;319(6):H1208-H1220. doi: 10.1152/ajpheart.00339.2020. Epub 2020 Sep 18. Am J Physiol Heart Circ Physiol. 2020. PMID: 32946260
-
Noninvasive Diagnostic Methods for Better Screening of Peripheral Arterial Disease.Ann Vasc Surg. 2018 Oct;52:263-272. doi: 10.1016/j.avsg.2018.03.018. Epub 2018 May 17. Ann Vasc Surg. 2018. PMID: 29777849 Review.
-
Optical techniques in the assessment of peripheral arterial disease.Curr Vasc Pharmacol. 2007 Jan;5(1):53-9. doi: 10.2174/157016107779317242. Curr Vasc Pharmacol. 2007. PMID: 17266613 Review.
Cited by
-
Validation of a New Ankle Brachial Index Measurement System Using Pulse Wave Velocity.Biosensors (Basel). 2024 May 16;14(5):251. doi: 10.3390/bios14050251. Biosensors (Basel). 2024. PMID: 38785725 Free PMC article.
-
The PROPHECI trial: a phase II, double-blind, placebo-controlled, randomized clinical trial for the treatment of pseudoxanthoma elasticum with oral pyrophosphate.Trials. 2025 Jan 29;26(1):30. doi: 10.1186/s13063-024-08666-w. Trials. 2025. PMID: 39881395 Free PMC article.
-
Set configuration influences cardiovascular responses to resistance exercise in postmenopausal females in a randomized crossover trial from the CARE project.Sci Rep. 2025 Aug 4;15(1):28373. doi: 10.1038/s41598-025-14379-0. Sci Rep. 2025. PMID: 40760080 Free PMC article. Clinical Trial.
References
-
- Cambou JP, Aboyans V, Constans J, Lacroix P, Dentans C, Bura A. Characteristics and outcome of patients hospitalised for lower extremity peripheral artery disease in France: the COPART Registry. Eur J Vasc Endovasc Surg 2010;39:577–585. - PubMed
-
- Association AD. Peripheral arterial disease in people with diabetes. Diabetes Care 2003;26:3333–3341. - PubMed
-
- Aboyans V, Criqui MH, Abraham P, Allison MA, Creager MA, Diehm C, Fowkes FGR, Hiatt WR, Jönsson B, Lacroix P, Marin B, McDermott MM, Norgren L, Pande RL, Preux P-M, Stoffers HE, Treat-Jacobson D. Measurement and interpretation of the ankle-brachial index: a scientific statement from the American Heart Association. Circulation 2012;126:2890–2909. - PubMed
-
- Herráiz-Adillo Á, Cavero-Redondo I, Álvarez-Bueno C, Martínez-Vizcaíno V, Pozuelo-Carrascosa DP, Notario-Pacheco B. The accuracy of an oscillometric ankle-brachial index in the diagnosis of lower limb peripheral arterial disease: a systematic review and meta-analysis. Int J Clin Pract 2017;71. - PubMed
LinkOut - more resources
Full Text Sources
