

Relationship of normal-weight central obesity with the risk for heart failure and atrial fibrillation: analysis of a nationwide health check-up and claims database
- PMID: 35919350
- PMCID: PMC9242061
- DOI: 10.1093/ehjopen/oeac026
Relationship of normal-weight central obesity with the risk for heart failure and atrial fibrillation: analysis of a nationwide health check-up and claims database
Abstract
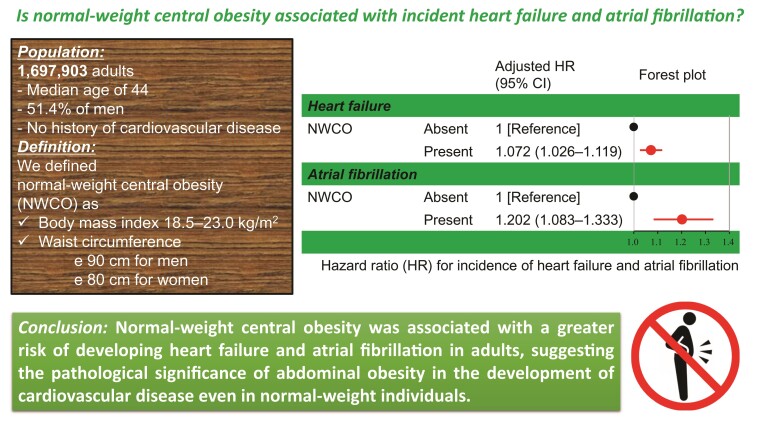
Aims: There have been scarce data on the relationship of normal-weight central obesity (NWCO) with the subsequent risk for heart failure (HF) and atrial fibrillation (AF). Using a nationwide health check-up and administrative claims database, we sought to clarify whether NWCO would be associated with the incidence of HF and AF.
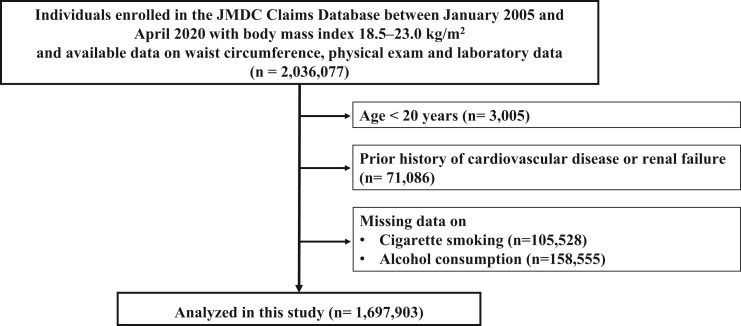
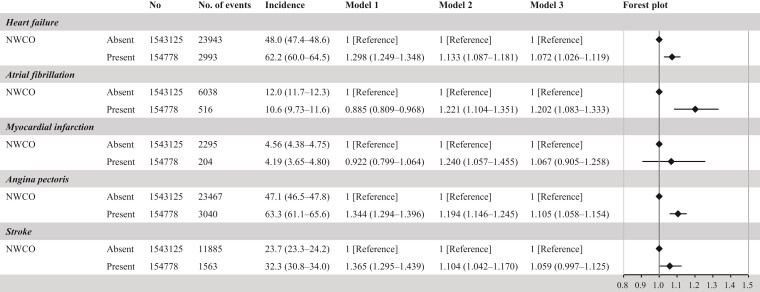
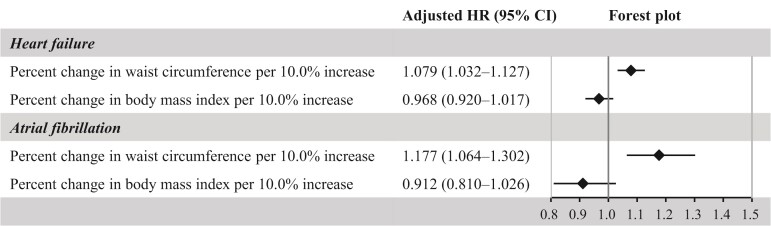
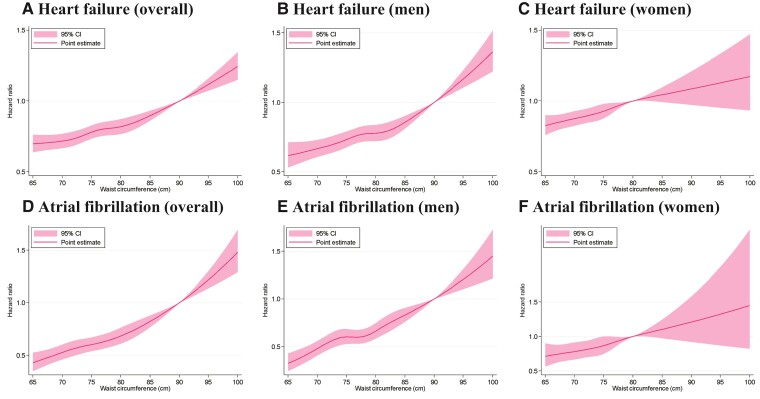
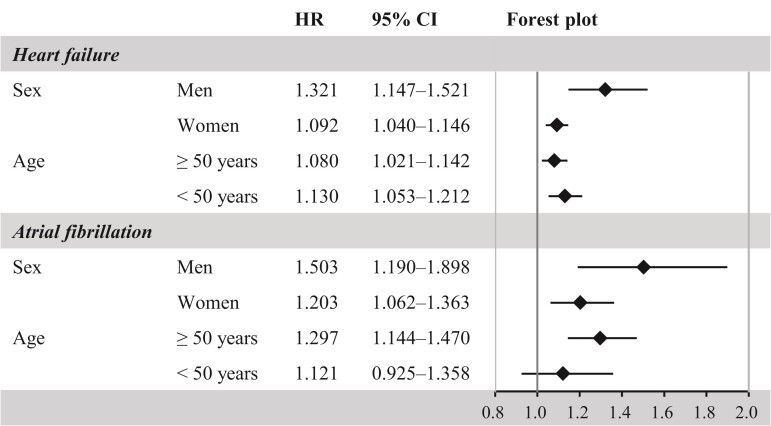
Methods and results: Medical records of 1 697 903 participants without prior history of cardiovascular disease (CVD) and normal-weight (body mass index of 18.5-23.0 kg/m2) were extracted from the JMDC Claims Database, which is a health check-up and claims database. We defined NWCO as normal-weight and CO (waist circumference ≥ 90 cm for men or ≥ 80 cm for women). The median age was 44.0 (37.0-52.0) years and 872 578 (51.4%) participants were men. Overall, 154 778 individuals (9.1%) had CO. The mean follow-up period was 3.3 ± 2.6 years. Participants with NWCO were older and more likely to be women than those without. HF and AF occurred in 26 936 (1.6%) and 6554 (0.4%) participants, respectively. People having NWCO were associated with a greater risk for HF [hazard ratio (HR): 1.072, 95% confidence interval (CI) 1.026-1.119] and AF (HR: 1.202, 95% CI: 1.083-1.333) compared with those having normal-weight without CO.
Conclusion: Our analysis of a nationwide health check-up and administrative claims database including ∼1.7 million participants without prevalent CVD history demonstrated the potential impact of NWCO on the risk for HF and AF, suggesting the importance of abdominal obesity in the developing HF and AF even in normal-weight individuals.
Keywords: Atrial fibrillation; Heart failure; Normal-weight central obesity; Preventive cardiology.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures


Similar articles
-
Association of Blood Pressure Classification Using the 2017 American College of Cardiology/American Heart Association Blood Pressure Guideline With Risk of Heart Failure and Atrial Fibrillation.Circulation. 2021 Jun 8;143(23):2244-2253. doi: 10.1161/CIRCULATIONAHA.120.052624. Epub 2021 Apr 22. Circulation. 2021. PMID: 33886370
-
Status and transition of normal-weight central obesity and the risk of cardiovascular diseases: A population-based cohort study in China.Nutr Metab Cardiovasc Dis. 2022 Dec;32(12):2794-2802. doi: 10.1016/j.numecd.2022.07.023. Epub 2022 Aug 9. Nutr Metab Cardiovasc Dis. 2022. PMID: 36319576
-
Familial hypercholesterolemia is related to cardiovascular disease, heart failure and atrial fibrillation. Results from a population-based study.Eur J Clin Invest. 2024 Feb;54(2):e14119. doi: 10.1111/eci.14119. Epub 2023 Nov 2. Eur J Clin Invest. 2024. PMID: 37916502
-
Cross-sectional study of associations between normal body weight with central obesity and hyperuricemia in Japan.BMC Endocr Disord. 2020 Jan 6;20(1):2. doi: 10.1186/s12902-019-0481-1. BMC Endocr Disord. 2020. PMID: 31906920 Free PMC article.
-
Relation of Serum Uric Acid and Cardiovascular Events in Young Adults Aged 20-49 Years.Am J Cardiol. 2021 Aug 1;152:150-157. doi: 10.1016/j.amjcard.2021.05.007. Epub 2021 Jun 14. Am J Cardiol. 2021. PMID: 34140140
Cited by
-
The Influence of Risk Factor Modification on Atrial Fibrillation Outcomes and Their Impact on the Success of Catheter Ablation.Rev Cardiovasc Med. 2025 Mar 21;26(3):27175. doi: 10.31083/RCM27175. eCollection 2025 Mar. Rev Cardiovasc Med. 2025. PMID: 40160571 Free PMC article. Review.
-
Evaluating waist-to-hip ratio in youth using frequency-modulated continuous wave radar and machine learning.Sci Rep. 2025 Jan 31;15(1):3911. doi: 10.1038/s41598-025-88098-x. Sci Rep. 2025. PMID: 39890860 Free PMC article.
-
Association of predicted body composition with occurrence of atrial fibrillation.Front Cardiovasc Med. 2023 Oct 10;10:1159087. doi: 10.3389/fcvm.2023.1159087. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37881721 Free PMC article.
-
Metabolic syndrome and cardiovascular disease in cancer survivors.J Cachexia Sarcopenia Muscle. 2024 Jun;15(3):1062-1071. doi: 10.1002/jcsm.13443. Epub 2024 Mar 22. J Cachexia Sarcopenia Muscle. 2024. PMID: 38515400 Free PMC article.
-
Higher childhood weight gain, lower skeletal muscle mass, and higher cereal consumption in normal-weight Japanese women with high-percentage trunk fat: a subanalysis study.Diabetol Int. 2023 Nov 7;15(2):194-202. doi: 10.1007/s13340-023-00670-w. eCollection 2024 Apr. Diabetol Int. 2023. PMID: 38524938 Free PMC article.
References
-
- Rexrode KM, Carey VJ, Hennekens CH, Walters EE, Colditz GA, Stampfer MJ, Willett WC, Manson JE. Abdominal adiposity and coronary heart disease in women. JAMA 1998;280:1843–1848. - PubMed
-
- Folsom AR, Stevens J, Schreiner PJ, McGovern PG. Body mass index, waist/hip ratio, and coronary heart disease incidence in African Americans and whites. Atherosclerosis risk in communities study investigators. Am J Epidemiol 1998;148:1187–1194. - PubMed
-
- Lakka HM, Lakka TA, Tuomilehto J, Salonen JT. Abdominal obesity is associated with increased risk of acute coronary events in men. Eur Heart J 2002;23:706–713. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
