

Hypernatremia in Hospitalized Patients: A Large Population-Based Study
- PMID: 35919520
- PMCID: PMC9337903
- DOI: 10.34067/KID.0000702022
Hypernatremia in Hospitalized Patients: A Large Population-Based Study
Abstract
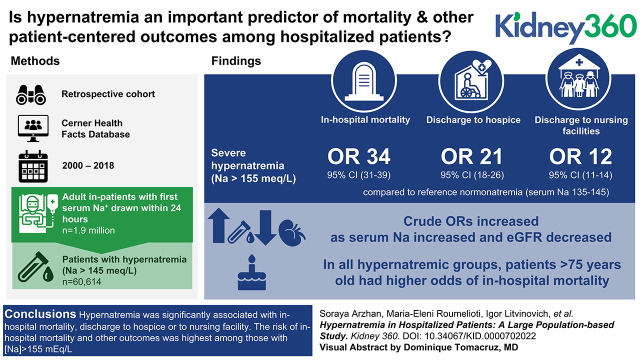
Background: Hypernatremia is a frequently encountered electrolyte disorder in hospitalized patients. Controversies still exist over the relationship between hypernatremia and its outcomes in hospitalized patients. This study examines the relationship of hypernatremia to outcomes among hospitalized patients and the extent to which this relationship varies by kidney function and age.
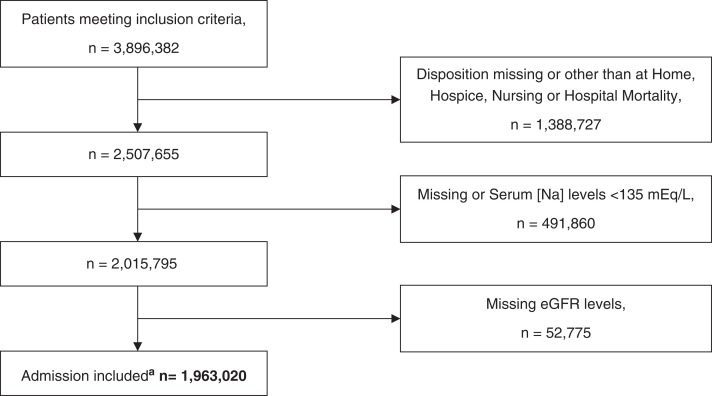
Methods: We conducted an observational study to investigate the association between hypernatremia, eGFR, and age at hospital admission and in-hospital mortality, and discharge dispositions. We analyzed the data of 1.9 million patients extracted from the Cerner Health Facts databases (2000-2018). Adjusted multinomial regression models were used to estimate the relationship of hypernatremia to outcomes of hospitalized patients.
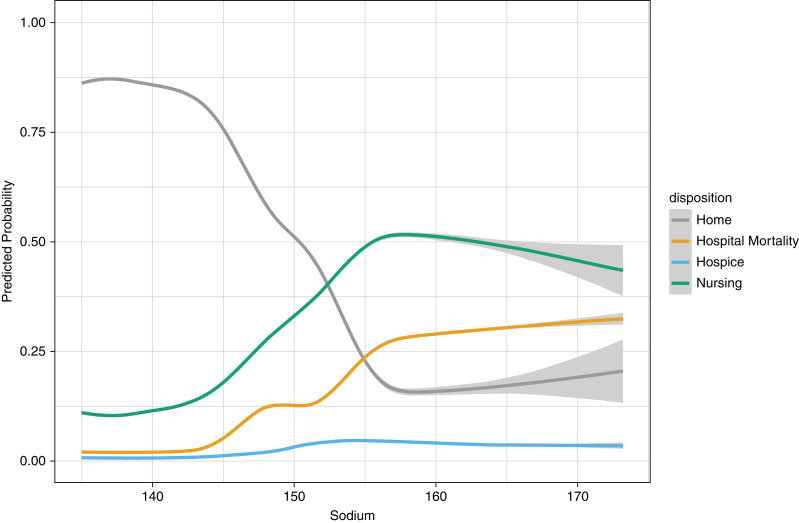
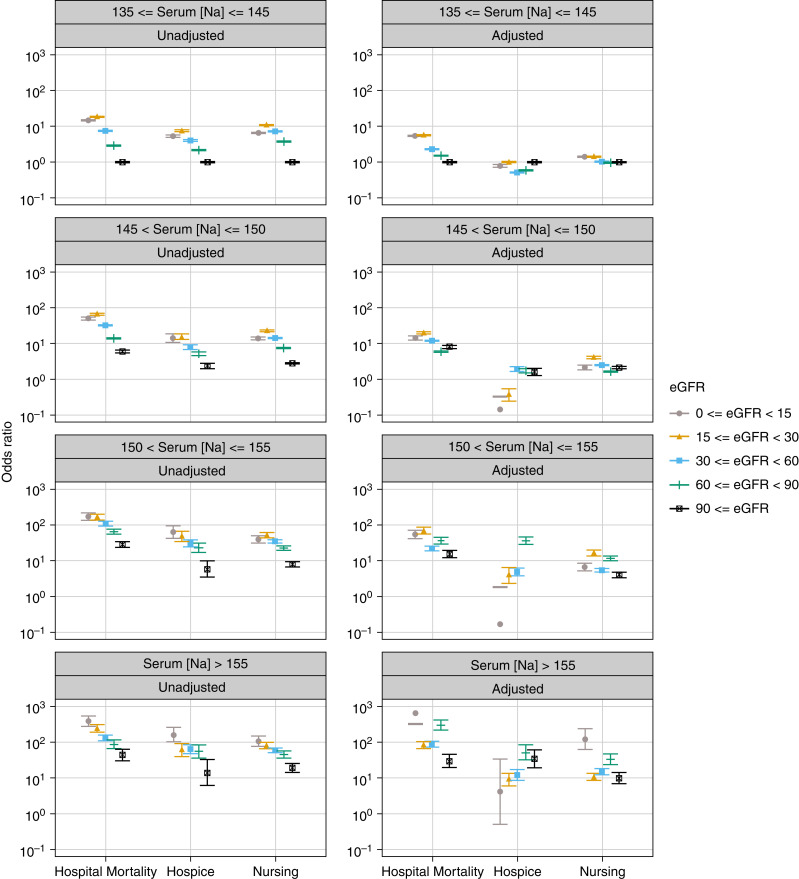
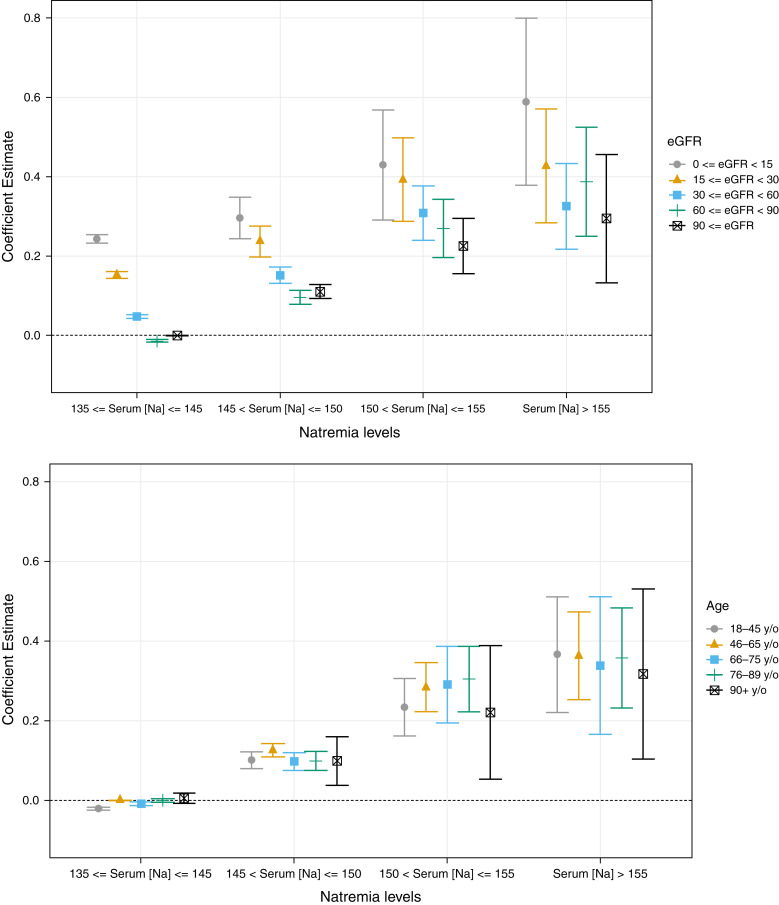
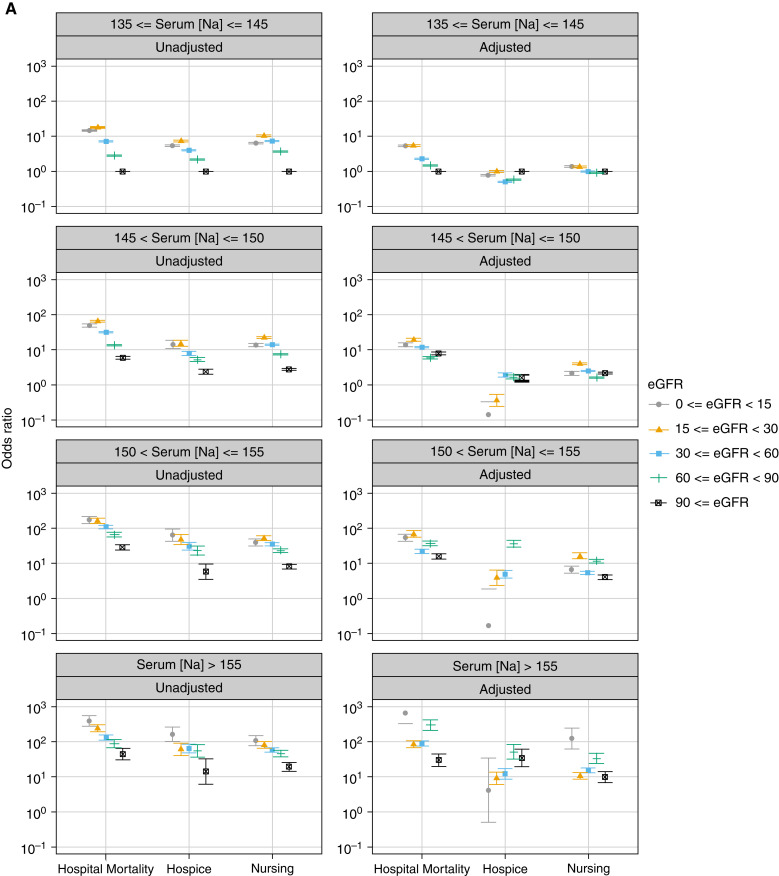
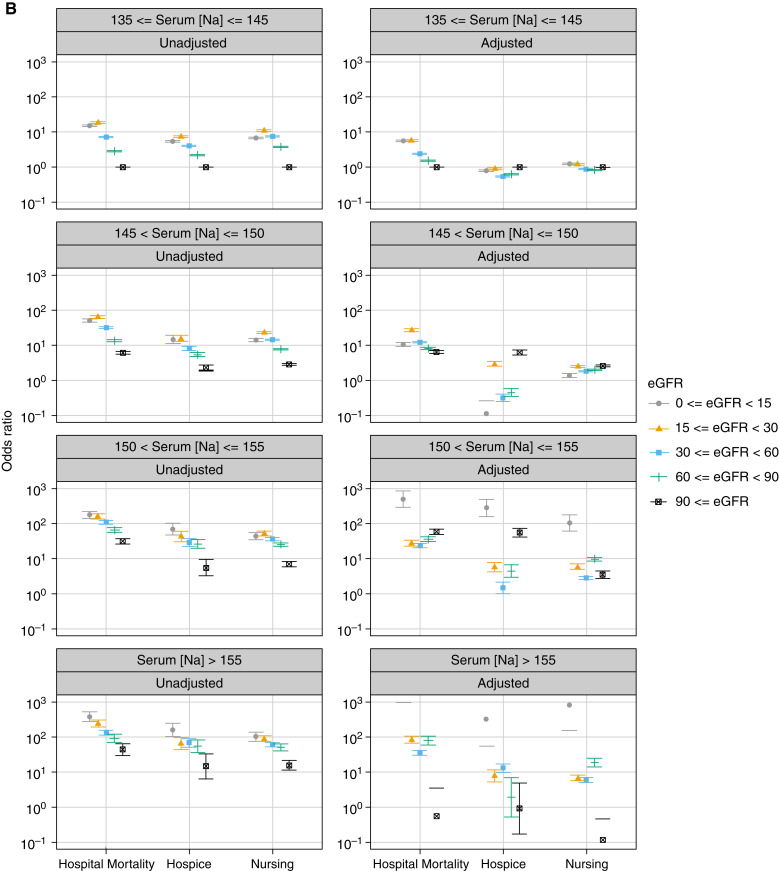
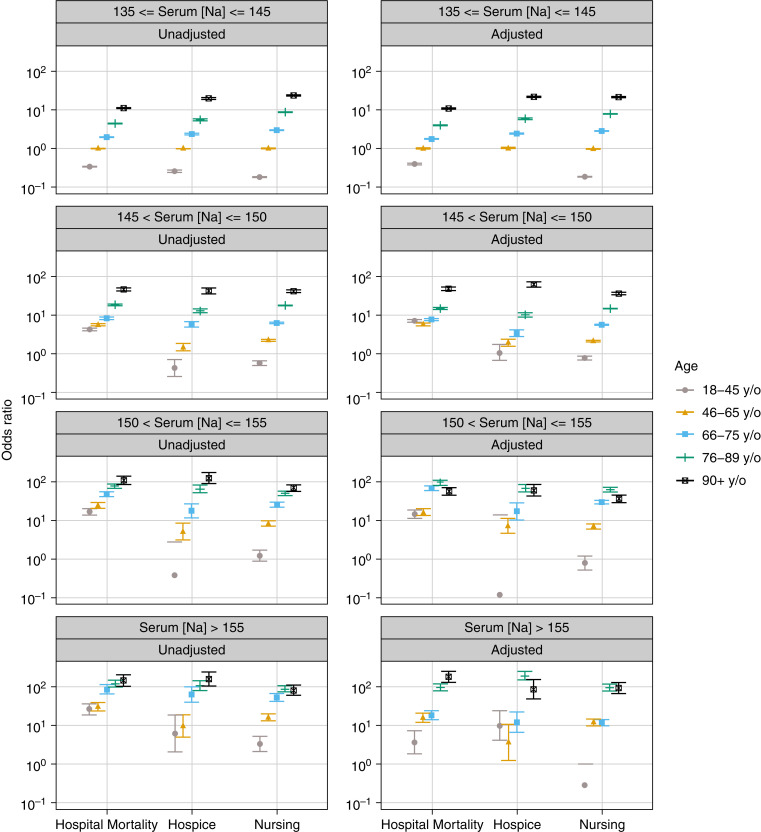
Results: Of all hospitalized patients, 3% had serum sodium (Na) >145 mEq/L at hospital admission. Incidence of in-hospital mortality was 12% and 2% in hyper- and normonatremic patients, respectively. The risk of all outcomes increased significantly for Na >155 mEq/L compared with the reference interval of Na=135-145 mEq/L. Odds ratios (95% confidence intervals) for in-hospital mortality and discharge to a hospice or nursing facility were 34.41 (30.59-38.71), 21.14 (17.53-25.5), and 12.21 (10.95-13.61), respectively (all P<0.001). In adjusted models, we found that the association between Na and disposition was modified by eGFR (P<0.001) and by age (P<0.001). Sensitivity analyses were performed using the eGFR equation without race as a covariate, and the inferences did not substantially change. In all hypernatremic groups, patients aged 76-89 and ≥90 had higher odds of in-hospital mortality compared with younger patients (all P<0.001).
Conclusions: Hypernatremia was significantly associated with in-hospital mortality and discharge to a hospice or nursing facility. The risk of in-hospital mortality and other outcomes was highest among those with Na >155 mEq/L. This work demonstrates that hypernatremia is an important factor related to discharge disposition and supports the need to study whether protocolized treatment of hypernatremia improves outcomes.
Keywords: chronic kidney disease; hypernatremia; mortality; outcomes.
Copyright © 2022 by the American Society of Nephrology.
Conflict of interest statement
M.L. Unruh reports consultancy for Cara Therapeutics to chair of Data Monitoring Committee; a consulting agreement between Cara and the University of New Mexico; research funding from Dialysis Clinic, Inc.; and honoraria from the American Society of Nephrology, NKF, and the Renal Research Institute related to lectures. M.-E. Roumelioti reports participating in Dialysis Clinic, Inc., quality meetings and receiving financial support. All remaining authors have nothing to disclose.
Figures
Comment in
-
Outcomes Associated with Hypernatremia at Admission in Hospitalized Persons.Kidney360. 2022 Jul 28;3(7):1122-1123. doi: 10.34067/KID.0003052022. eCollection 2022 Jul 28. Kidney360. 2022. PMID: 35919539 Free PMC article. No abstract available.
References
-
- Tsipotis E, Price LL, Jaber BL, Madias NE: Hospital-associated hypernatremia spectrum and clinical outcomes in an unselected cohort. Am J Med 131: 72–82.e1, 2018 - PubMed
-
- Lombardi G, Ferraro PM, Calvaruso L, Naticchia A, D’Alonzo S, Gambaro G: Sodium fluctuations and mortality in a general hospitalized population. Kidney Blood Press Res 44: 604–614, 2019 - PubMed
-
- Jung WJ, Lee HJ, Park S, Lee SN, Kang HR, Jeon JS, Noh H, Han DC, Kwon SH: Severity of community acquired hypernatremia is an independent predictor of mortality. Intern Emerg Med 12: 935–940, 2017. 28474207 - PubMed
-
- Akirov A, Diker-Cohen T, Steinmetz T, Amitai O, Shimon I: Sodium levels on admission are associated with mortality risk in hospitalized patients. Eur J Int Med 46: 25–29, 2017 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
