

Inflammatory bowel disease and cardiovascular diseases: a concise review
- PMID: 35919661
- PMCID: PMC9242064
- DOI: 10.1093/ehjopen/oeab029
Inflammatory bowel disease and cardiovascular diseases: a concise review
Abstract
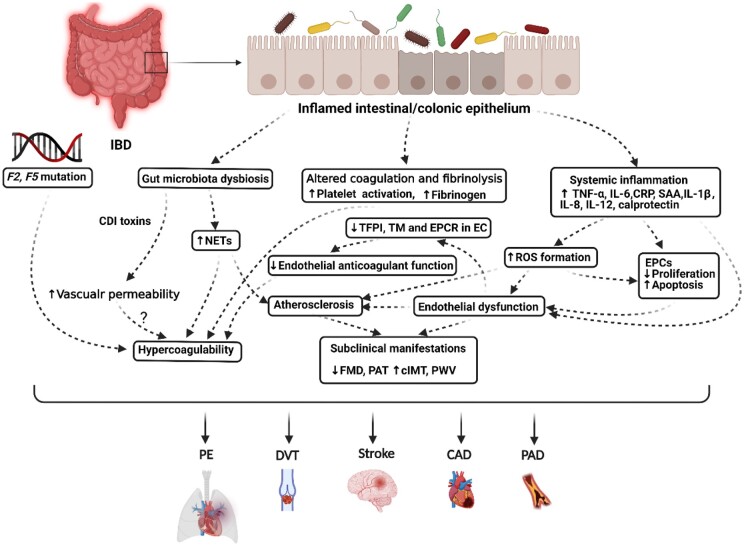
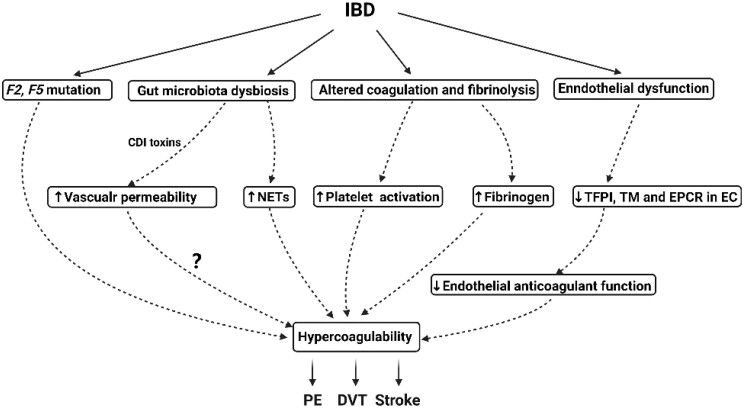
Cardiovascular diseases (CVDs) remain the leading cause of morbidity and mortality despite aggressive treatment of traditional risk factors. Chronic inflammation plays an important role in the initiation and progression of CVDs. Inflammatory bowel disease (IBD) is a systemic state of inflammation exhibiting increased levels of pro-inflammatory cytokines including tumour necrosis factor-α (TNF-α), interleukin (IL)-1β, and IL-6. Importantly, IBD is associated with increased risk for CVDs especially in women and young adults, including coronary artery disease, stroke, thromboembolic diseases, and arrhythmias. Potential mechanisms underlying the increased risk for CVDs in IBD patients include increased levels of inflammatory cytokines and oxidative stress, altered platelet function, hypercoagulability, decreased numbers of circulating endothelial progenitor cells, endothelial dysfunction, and possible interruption of gut microbiota. Although IBD does not appear to exacerbate the traditional risk factors for CVDs, including hypertension, hyperlipidaemia, diabetes mellitus, and obesity, aggressive risk stratifications are important for primary and secondary prevention of CVDs for IBD patients. Compared to 5-aminosalicylates and corticosteroids, anti-TNF-α therapy in IBD patients was consistently associated with decreasing cardiovascular events. In the absence of contraindications, low-dose aspirin and statins appear to be beneficial for IBD patients. Low-molecular-weight heparin is also recommended for patients who are hospitalized with acute IBD flares without major bleeding risk. A multidisciplinary team approach should be considered for the management of IBD patients.
Keywords: Cardiovascular medications; Inflammatory bowel disease; Ischaemic arterial disease; Venous thromboembolism.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

References
-
- Roifman I, Sun YC, Fedwick JP, Panaccione R, Buret AG, Liu H, Rostom A, Anderson TJ, Beck PL. Evidence of endothelial dysfunction in patients with inflammatory bowel disease. Clin Gastroenterol Hepatol 2009;7:175–182. - PubMed
-
- Kirchgesner J, Beaugerie L, Carrat F, Andersen NN, Jess T, Schwarzinger M; BERENICE study group. Increased risk of acute arterial events in young patients and severely active IBD: a nationwide French cohort study. Gut 2018;67:1261–1268. - PubMed
-
- Grainge MJ, West J, Card TR. Venous thromboembolism during active disease and remission in inflammatory bowel disease: a cohort study. Lancet 2010;375:657–663. - PubMed
LinkOut - more resources
Full Text Sources
