Role of early decompressive craniectomy in traumatic brain injury: Our clinical experience
- PMID: 35920418
- PMCID: PMC10315979
- DOI: 10.14744/tjtes.2021.23176
Role of early decompressive craniectomy in traumatic brain injury: Our clinical experience
Abstract
Background: Traumatic brain injury (TBI) is an important cause of death, especially in underdeveloped and developing countries. Diffuse edema in the damaged cerebral tissue as a result of trauma and the subsequent increase in intracranial pressure cause signifi-cant neurological deterioration. Consequently, decompressive craniectomy (DC) is performed as the surgical treatment of TBI. The aim of this study is to evaluate the post-operative mortality and morbidity rates of patients who underwent DC for TBI in our clinic.
Methods: The data of 57 cases of TBI were retrospectively analyzed. Clinical, radiological and surgical features of these cases were reviewed. The rates of mortality and morbidity, as well as main indicators of mortality were investigated.
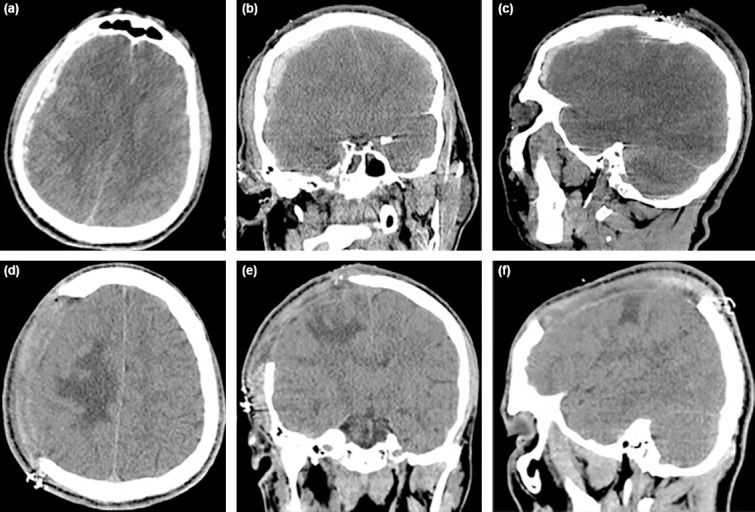
Results: Twenty-five (43.8%) patients were female and 32 (56.1%) were male. The mean age was 54.5 years. Fourteen (24.5%) patients were presented with subdural hematoma, 5 (8.7%) with epidural hematoma, 18 (31.5%) with intracerebral hematoma, 13 (22.8%) with subarachnoid hemorrhage, and 7 (12.2%) with other radiological findings. DC was performed in all cases as soon as pos-sible after admission. Twelve (21.1%) patients died in the first 3 days postoperatively and 7 (12.2%) patients in the postoperative 3-15 days due to progressive cerebral damage and secondary infections. Six (10.5%) patients recovered completely and were discharged. Thirty-two (56.1%) patients were transferred to palliative care clinics and physical therapy clinics after the surgical treatment.
Conclusion: DC, which is performed in the early period of treatment in TBI, is as important as the degree of intracerebral damage at the time of admission and the high Glasgow coma scale score. Post-operative results are more satisfactory in patients who underwent DC at an earlier stage of treatment.
Conflict of interest statement
Figures

Similar articles
-
An Analysis of Emergency Surgical Outcomes for Pediatric Traumatic Brain Injury: A Ten-Year Single-Institute Retrospective Study in Taiwan.Medicina (Kaunas). 2024 Sep 18;60(9):1518. doi: 10.3390/medicina60091518. Medicina (Kaunas). 2024. PMID: 39336560 Free PMC article.
-
Intracranial pressure in patients undergoing decompressive craniectomy: new perspective on thresholds.J Neurosurg. 2018 Mar;128(3):819-827. doi: 10.3171/2016.11.JNS162263. Epub 2017 Apr 14. J Neurosurg. 2018. PMID: 28409728
-
Decompressive craniectomy versus craniotomy only for intracranial hemorrhage evacuation: A propensity matched study.J Trauma Acute Care Surg. 2017 Dec;83(6):1148-1153. doi: 10.1097/TA.0000000000001658. J Trauma Acute Care Surg. 2017. PMID: 28715363
-
Decompressive craniectomy for severe traumatic brain injury in children: analysis of long-term neuropsychological impairment and review of the literature.Childs Nerv Syst. 2019 Sep;35(9):1507-1515. doi: 10.1007/s00381-019-04274-1. Epub 2019 Jul 1. Childs Nerv Syst. 2019. PMID: 31264065 Review.
-
Early Decompressive Craniectomy as Management for Severe Traumatic Brain Injury in the Pediatric Population: A Comprehensive Literature Review.World Neurosurg. 2020 Jun;138:9-18. doi: 10.1016/j.wneu.2020.02.065. Epub 2020 Feb 19. World Neurosurg. 2020. PMID: 32084616 Review.
References
-
- Cooper DJ, Rosenfeld JV, Murray L, Arabi YM, Davies AR, D'Urso P, et al. Decompressive craniectomy in diffuse traumatic brain ınjury. N Engl J Med. 2011;364:1493–502. - PubMed
-
- De Silva MJ, Roberts I, Perel P, Edwards P, Kenward MG, Fernandes J, et al. Patient outcome after traumatic brain injury in high, middle and low-income countries:Analysis of data on 8927 patients in 46 countries. Int J Epidemiol. 2009;38:452–8. - PubMed
-
- Solmaz I, Kural C, Temiz C, Seçer HI, Düz B, Gönül E, et al. Traumatic brain injury due to gunshot wounds:A single institution's experience with 442 consecutive patients. Turk Neurosurg. 2009;19:216–23. - PubMed
-
- Coronado VG, Xu L, Basavaraju SV, McGuire LC, Wald MM, Faul MD, et al. Surveillance for traumatic brain injury-related deaths-United States, 1997-2007. MMWR Surveill Summ. 2011;60(5):1–32. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical