Early movement does not cause loss of reduction in surgically treated boxer fractures
- PMID: 35920419
- PMCID: PMC10315983
- DOI: 10.14744/tjtes.2021.24668
Early movement does not cause loss of reduction in surgically treated boxer fractures
Abstract
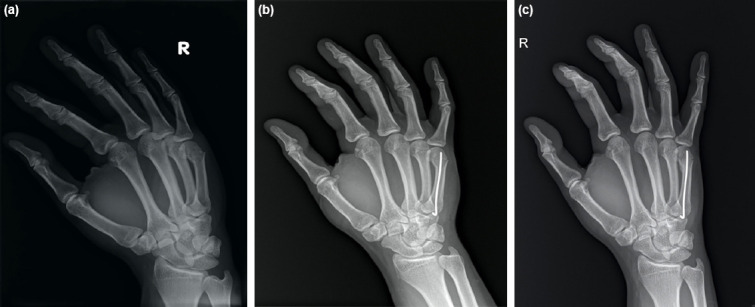
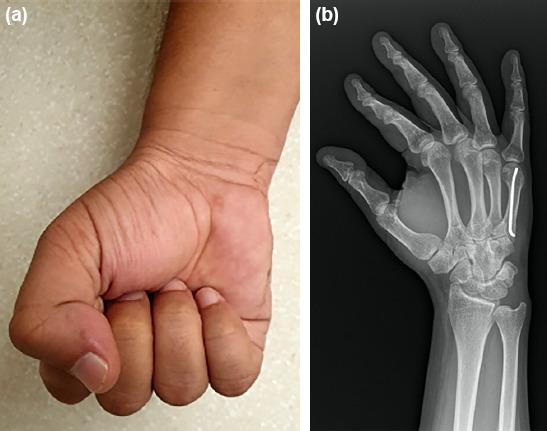
Background: The surgical treatment of fifth metacarpal fractures, especially using Kirschner (K) wire techniques, has recently become popular because it provides for early hand movement. Successful anatomical reduction of the fracture is often achieved with surgery; however, an anatomical reduction cannot always be achieved and, according to 30° oblique radiography, the fracture is fixed with an apex dorsal angulation below 40°. The aim of this study was to evaluate the stability of such fractures postoperatively and compare the two different angulation options that provide early movement of the hand and wrist.
Methods: Thirty consecutive cases of neck fractures of the fifth metacarpal were treated intramedullarly with one K wire. Cases were divided into two groups: One fixed with anatomical reduction (Group 1) and the other (Group 2) fixed in apex dorsal angulation below 40°, according to 30° oblique radiography. Angulation, shortening, and functional outcome as Quick DASH scores and grip strengths were evaluated at 6 months.
Results: The mean correction angle was 56.6° (between 30° and 110°) for Group 1 and the residual angle was 0°. The mean cor-rection angle was 42.4° (between 20° and 75°) for group 2 (Figs. 4 and 5) and the residual angle was 23.6° (between 10° and 45°). The mean Quick DASH scores were 1.9 (SD: 1.7) for Group 1 and 5.67 (SD: 2.93) for Group 2 (p<0.05). Grip strength values were similar for both groups. All the patients returned to their previous occupations without any limitations in an average of 4 weeks (SD: 1.4) (range 2-6 weeks). No complications such as correction loosening or shortening were detected. Rotation was not detected during physical examination.
Conclusion: Our investigation revealed no risk of shortening or rotation of the fracture; the patients were able to return quickly to their everyday activities.
Conflict of interest statement
Figures

Similar articles
-
Antegrade intramedullary pinning versus retrograde intramedullary pinning for displaced fifth metacarpal neck fractures.Clin Orthop Relat Res. 2015 May;473(5):1747-54. doi: 10.1007/s11999-014-4079-7. Epub 2014 Dec 11. Clin Orthop Relat Res. 2015. PMID: 25502343 Free PMC article. Clinical Trial.
-
Modified retrograde percutaneous intramedullary multiple Kirschner wire fixation for treatment of unstable displaced metacarpal neck and shaft fractures.Eur J Orthop Surg Traumatol. 2013 Jul;23(5):535-43. doi: 10.1007/s00590-012-1036-6. Epub 2012 Jul 7. Eur J Orthop Surg Traumatol. 2013. PMID: 23412169
-
Results of surgical treatment in metacarpal shaft fractures using low profile mini plates.Ulus Travma Acil Cerrahi Derg. 2015 Jul;21(4):279-84. doi: 10.5505/tjtes.2015.01651. Ulus Travma Acil Cerrahi Derg. 2015. PMID: 26374415
-
Extraarticular hand fractures in adults: a review of new developments.Clin Orthop Relat Res. 2006 Apr;445:133-45. doi: 10.1097/01.blo.0000205888.04200.c5. Clin Orthop Relat Res. 2006. PMID: 16505726 Review.
-
Challenging the dogma: severely angulated neck fractures of the fifth metacarpal must be treated surgically.J Hand Surg Eur Vol. 2021 Jan;46(1):30-36. doi: 10.1177/1753193420968040. Epub 2020 Nov 1. J Hand Surg Eur Vol. 2021. PMID: 33135525
References
-
- Memon FW, Patankar H, Nagori AM. “Bouquet technique”for displaced boxers fracture:Surgical technique and outcomes in 143 consecutive cases. Int J Biomed Res. 2018;9:202–7.
-
- Cepni SK, Aykut S, Bekmezci T, Kilic A. A minimally invasive fixation technique for selected patients with fifth metacarpal neck fracture. Injury. 2016;47:1270–5. - PubMed
-
- Boeckstyns ME. Challenging the dogma:severely angulated neck fractures of the fifth metacarpal must be treated surgically. J Hand Surg Eur Vol. 2021;46:30–6. - PubMed
-
- Marsh JL, Slongo TF, Agel J, Broderick JS, Creevey W, DeCoster TA, et al. Fracture and dislocation classification compendium -2007:Orthopaedic Trauma Association classification, database and outcomes committee. J Orthop Trauma. 2007;21:S1–133. - PubMed
-
- Sokolove PE, Barnes DK. Clinical procedures in emergency medicine. Philadelphia: Saunders; 2004. Extensor and flexor tendon injuries in the hand, wrist, and foot.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous