The clinical feature and outcome of groove pancreatitis in a cohort: A single center experience with review of the literature
- PMID: 35920434
- PMCID: PMC10315977
- DOI: 10.14744/tjtes.2022.12893
The clinical feature and outcome of groove pancreatitis in a cohort: A single center experience with review of the literature
Abstract
Background: Groove pancreatitis (GP) is a rare form of chronic pancreatitis that is less common and is now gaining awareness with multimodal imaging modalities. Our aim is to analyze the mid-long term outcomes of patients diagnosed with GP with different treatment approaches.
Methods: A computerized search from electronic patient record database between May 2013 and June 2019 with the keywords 'groove', 'paraduodenal' was applied. The clinical, radiological and pathological data of 25 patients diagnosed with GP were obtained.
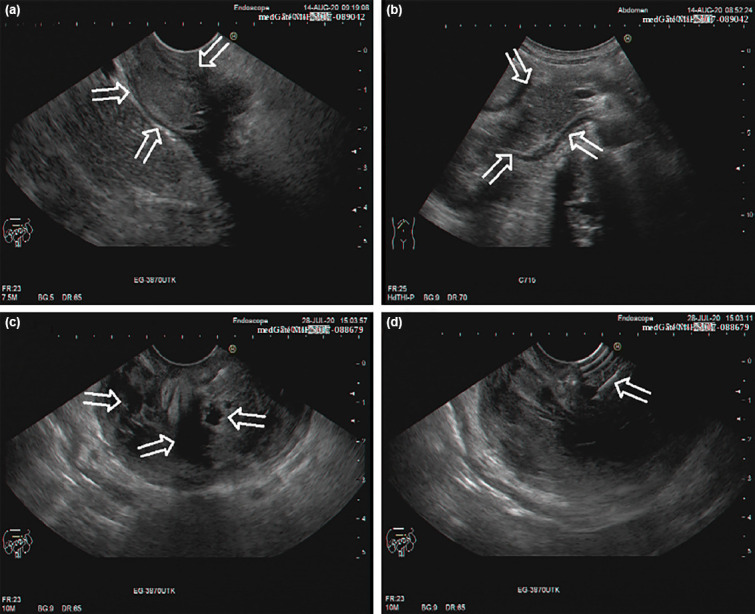
Results: In the GP patient group, the median age was 55 (25-87) and 80% was male. Alcohol and tobacco abuse was 40% among GP patients. The most common symptoms were upper abdominal pain (84%) and nausea-vomiting (40%), respectively. Gastric outlet obstruction was observed in 4 (16%) patients. CT and EUS imaging were performed to majority of cases (96% and 92 %, respectively). EUS-FNA was done in 14 of 25 (56%) patients. It was reported as atypia, adenocarcinoma and benign in 2 (8%), 2 (8%) and 10 (40%) patients, respectively. EUS-FNA was helpful to diagnose two pancreatic head adenoCA whose preliminary radiological evaluation was GP. The mean follow-up period was 29 (3-71) months. Conservative approach was the predominantly preferred treatment (%56). Apart from conservative approach, treatment strategies included biliary stenting, sphincterotomy, wirsung stenting via ERCP, cholecystectomy etc. Considering all treatment modalities, symptoms improved in 12 (48%) patients and progressed with recurrent pancreatitis attacks in 7 (28%) patients.
Conclusion: Because GP is a less well-known form of pancreatitis, it presents several challenges for clinicians in diagnosis and treatment. This form, which can mimic pancreatic malignancy in particular, must be differentiated from carcinoma. EUS(±FNA) is a useful diagnostic tool complementary to imaging. Although the conservative approach remains the first choice in most patients, the clinician should consider invasive endoscopic procedures and surgical options in special cases when necessary.
Conflict of interest statement
Figures

Similar articles
-
Diagnostic value of endoscopic ultrasound in groove pancreatitis.Ann Med. 2023;55(2):2295991. doi: 10.1080/07853890.2023.2295991. Epub 2023 Dec 22. Ann Med. 2023. PMID: 38134890 Free PMC article. Review.
-
Comparison between groove carcinoma and groove pancreatitis.Pancreatology. 2018 Oct;18(7):805-811. doi: 10.1016/j.pan.2018.08.013. Epub 2018 Aug 30. Pancreatology. 2018. PMID: 30224296
-
Predictors of Malignancies in Patients with Inconclusive or Negative Results of Endoscopic Ultrasound-guided Fine-needle Aspiration for Solid Pancreatic Masses.Korean J Gastroenterol. 2018 Mar 25;71(3):153-161. doi: 10.4166/kjg.2018.71.3.153. Korean J Gastroenterol. 2018. PMID: 29566476
-
The effectiveness of a conservative approach in the management of groove pancreatitis.Indian J Gastroenterol. 2025 Jan 18. doi: 10.1007/s12664-024-01715-x. Online ahead of print. Indian J Gastroenterol. 2025. PMID: 39826079
-
Groove pancreatitis vs groove pancreatic adenocarcinoma. Report of two cases and review of the literature.Acta Gastroenterol Latinoam. 2013 Sep;43(3):248-53. Acta Gastroenterol Latinoam. 2013. PMID: 24303693 Review.
Cited by
-
Diagnostic value of endoscopic ultrasound in groove pancreatitis.Ann Med. 2023;55(2):2295991. doi: 10.1080/07853890.2023.2295991. Epub 2023 Dec 22. Ann Med. 2023. PMID: 38134890 Free PMC article. Review.
-
Paraduodenal pancreatitis as diagnostic challenge: clinical and morphological features of patients with pancreatic pathology involving the pancreatic groove.Ann Gastroenterol. 2024 Nov-Dec;37(6):742-749. doi: 10.20524/aog.2024.0914. Epub 2024 Oct 20. Ann Gastroenterol. 2024. PMID: 39568705 Free PMC article.
-
Imaging of paraduodenal pancreatitis: A systematic review.World J Radiol. 2023 Feb 28;15(2):42-55. doi: 10.4329/wjr.v15.i2.42. World J Radiol. 2023. PMID: 36874260 Free PMC article.
-
Systematic review on groove pancreatitis: management of a rare disease.BJS Open. 2023 Sep 5;7(5):zrad094. doi: 10.1093/bjsopen/zrad094. BJS Open. 2023. PMID: 37749756 Free PMC article.
-
Surgical Management of Groove Pancreatitis: Lessons Learnt and Long-Term Experience.Dig Dis Sci. 2025 Jul;70(7):2521-2533. doi: 10.1007/s10620-025-09025-8. Epub 2025 Apr 9. Dig Dis Sci. 2025. PMID: 40205281
References
-
- Casetti L, Bassi C, Salvia R, Butturini G, Graziani R, Falconi M, et al. “Paraduodenal”pancreatitis:Results of surgery on 58 consecutives patients from a single institution. World J Surg. 2009;33:2664–9. - PubMed
-
- Becker V, Mischke U. Groove pancreatitis. Int J Pancreatol. 1991;10:173–82. - PubMed
-
- Shudo R, Obara T, Tanno S, Fujii T, Nishino N, Sagawa M, et al. Segmental groove pancreatitis accompanied by protein plugs in Santorini's duct. J Gastroenterol. 1998;33:289–94. - PubMed
-
- Adsay NV, Zamboni G. Paraduodenal pancreatitis:A clinico-pathologically distinct entity unifying “cystic dystrophy of heterotopic pancreas”, “para-duodenal wall cyst”, and “groove pancreatitis”. Semin Diagn Pathol. 2004;21:247–54. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical