

Association between hypotension and myocardial injury in patients with severe trauma
- PMID: 35920849
- PMCID: PMC9925499
- DOI: 10.1007/s00068-022-02051-5
Association between hypotension and myocardial injury in patients with severe trauma
Abstract
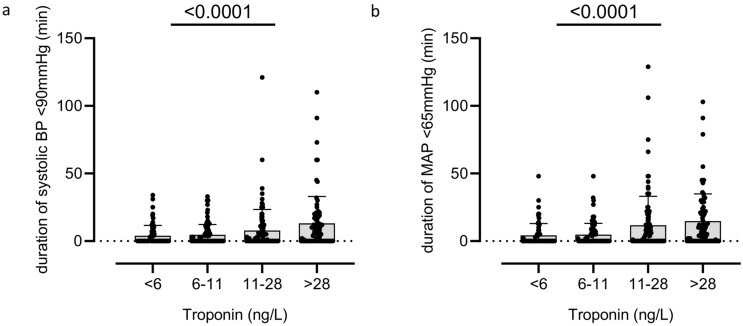
Purpose: During resuscitation of patients with severe trauma, guidelines recommend permissive hypotension prior to surgical bleeding control. However, hypotension may be associated with reduced organ perfusion and multiple organ dysfunction, e.g. myocardial injury. The association between hypotension and myocardial injury in trauma patients is underexplored. We hypothesized that hypotension is associated with myocardial injury in this population.
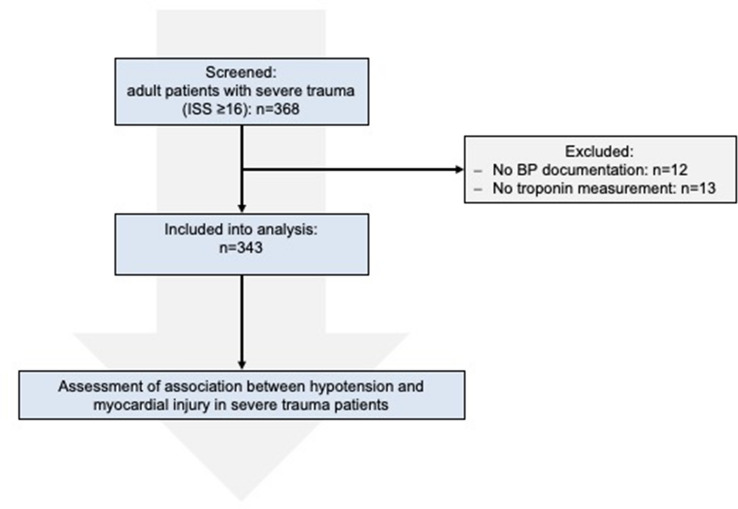
Materials and methods: This retrospective study included patients ≥ 18 years suffering from severe trauma [defined as Injury Severity Score (ISS) ≥ 16] that were treated in the emergency department resuscitation room between 2016 and 2019. Primary endpoint was the incidence of myocardial injury defined as high-sensitive troponin T > 14 ng/l. Main exposure was the duration of arterial hypotension during resuscitation period defined as mean arterial pressure < 65 mmHg.
Results: Out of 368 patients screened, 343 were analyzed (73% male, age: 55 ± 21, ISS: 28 ± 12). Myocardial injury was detected in 143 (42%) patients. Overall in-hospital mortality was 26%. Multivariate binary logistic regression with forced entry of nine predefined covariables revealed an odds ratio of 1.29 [95% confidence interval 1.16-1.44]; p = 0.012) for the association between the duration of hypotension and myocardial injury.
Conclusion: The duration of hypotension during resuscitation period is independently associated with the incidence of myocardial injury in patients with severe trauma.
Keywords: Blood pressure; Hemodynamics; Mean arterial pressure; Multiple trauma; Permissive hypotension; Troponin.
© 2022. The Author(s).
Conflict of interest statement
All authors declare that there are no conflicts of interest.
Figures
Similar articles
-
Incidence and prognosis of myocardial injury in patients with severe trauma.Eur J Trauma Emerg Surg. 2022 Aug;48(4):3073-3079. doi: 10.1007/s00068-021-01846-2. Epub 2021 Dec 8. Eur J Trauma Emerg Surg. 2022. PMID: 34878581 Free PMC article.
-
Prehospital management and fluid resuscitation in hypotensive trauma patients admitted to Karolinska University Hospital in Stockholm.Prehosp Disaster Med. 2005 Jul-Aug;20(4):228-34. doi: 10.1017/s1049023x00002582. Prehosp Disaster Med. 2005. PMID: 16128470
-
Prehospital times and outcomes of patients who had hypotension at the scene after trauma: A nationwide multicentre retrospective study.Injury. 2020 May;51(5):1224-1230. doi: 10.1016/j.injury.2020.02.002. Epub 2020 Feb 5. Injury. 2020. PMID: 32057459
-
Permissive hypotension versus conventional resuscitation strategies in adult trauma patients with hemorrhagic shock: A systematic review and meta-analysis of randomized controlled trials.J Trauma Acute Care Surg. 2018 May;84(5):802-808. doi: 10.1097/TA.0000000000001816. J Trauma Acute Care Surg. 2018. PMID: 29370058
-
Permissive hypotension/hypotensive resuscitation and restricted/controlled resuscitation in patients with severe trauma.J Intensive Care. 2017 Jan 20;5(1):11. doi: 10.1186/s40560-016-0202-z. J Intensive Care. 2017. PMID: 34798698 Free PMC article. Review.
Cited by
-
Coronary artery calcification detected by initial polytrauma CT in severely injured patients: retrospective single-center cohort study.Eur J Trauma Emerg Surg. 2024 Aug;50(4):1527-1536. doi: 10.1007/s00068-024-02487-x. Epub 2024 Mar 5. Eur J Trauma Emerg Surg. 2024. PMID: 38441580 Free PMC article.
-
A comprehensive review of massive transfusion and major hemorrhage protocols: origins, core principles and practical implementation.Braz J Anesthesiol. 2025 Mar-Apr;75(2):844583. doi: 10.1016/j.bjane.2024.844583. Epub 2024 Dec 25. Braz J Anesthesiol. 2025. PMID: 39730103 Free PMC article. Review.
-
Door-to-Balloon Time and Clinical Outcome of Patients Presenting with ST-Segment Elevation Myocardial Infarction During on and off Hours: a Single Center Study.Med Arch. 2025;79(3):172-180. doi: 10.5455/medarh.2025.79.172-180. Med Arch. 2025. PMID: 40657341 Free PMC article.
-
Impact of severe splenic trauma and its management on the occurrence of infections in intensive care unit.Trauma Surg Acute Care Open. 2025 Jul 1;10(3):e001704. doi: 10.1136/tsaco-2024-001704. eCollection 2025. Trauma Surg Acute Care Open. 2025. PMID: 40612645 Free PMC article.
-
Comparison of safety and efficacy of thoracic epidural block and erector spinae plane block for analgesia in patients with multiple rib fractures: A pilot single-blinded, randomised controlled trial.Indian J Anaesth. 2023 Jul;67(7):614-619. doi: 10.4103/ija.ija_844_21. Epub 2023 Jul 14. Indian J Anaesth. 2023. PMID: 37601936 Free PMC article.
References
-
- Salmasi V, Maheshwari K, Yang D, et al. Relationship between intraoperative hypotension, defined by either reduction from baseline or absolute thresholds, and acute kidney and myocardial injury after noncardiac surgery: a retrospective cohort analysis. Anesthesiology. 2017;126(1):47–65. doi: 10.1097/ALN.0000000000001432. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
