

Trends in osteoporosis care patterns during the COVID-19 pandemic in Alberta, Canada
- PMID: 35920939
- PMCID: PMC9349101
- DOI: 10.1007/s11657-022-01132-7
Trends in osteoporosis care patterns during the COVID-19 pandemic in Alberta, Canada
Abstract
Purpose/introduction: The objective of this study was to describe osteoporosis-related care patterns during the coronavirus disease 2019 (COVID-19) pandemic in Alberta, Canada, relative to the 3-year preceding.
Methods: A repeated cross-sectional study design encompassing 3-month periods of continuous administrative health data between March 15, 2017, and September 14, 2020, described osteoporosis-related healthcare resource utilization (HCRU) and treatment patterns. Outcomes included patients with osteoporosis-related healthcare encounters, physician visits, diagnostic and laboratory test volumes, and treatment initiations and disruptions. The percent change between outcomes was calculated, averaged across the control periods (2017-2019), relative to the COVID-19 periods (2020).
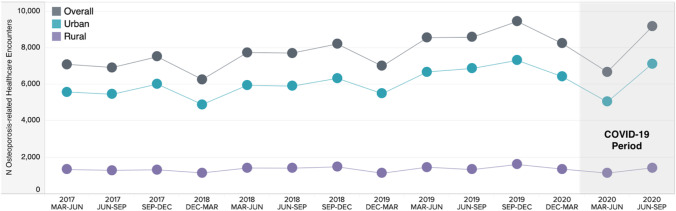
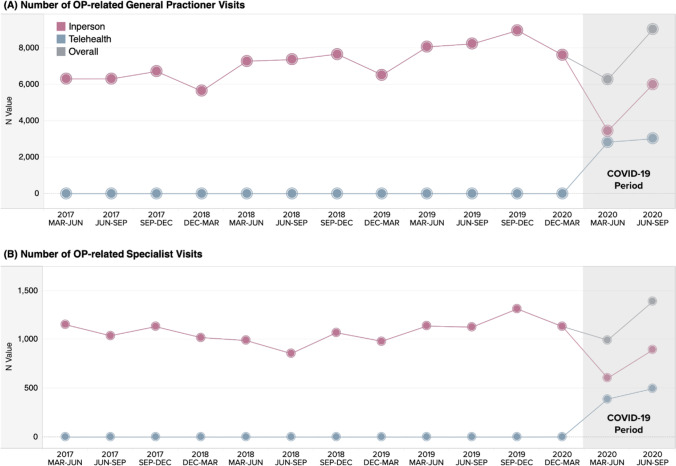
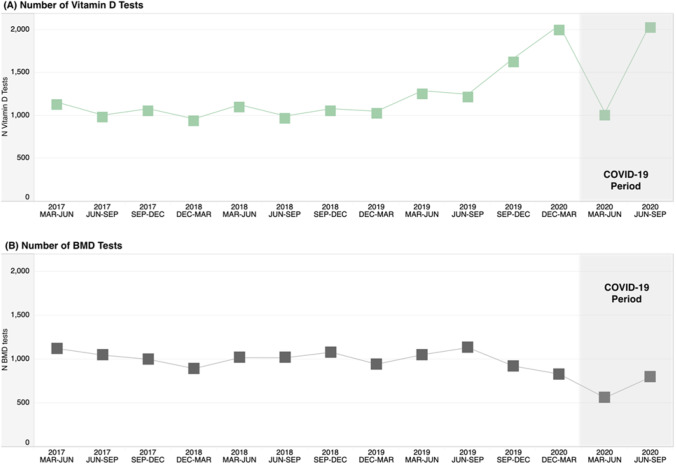
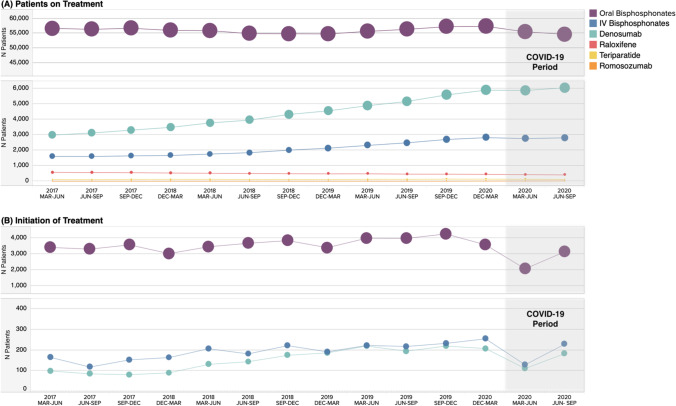
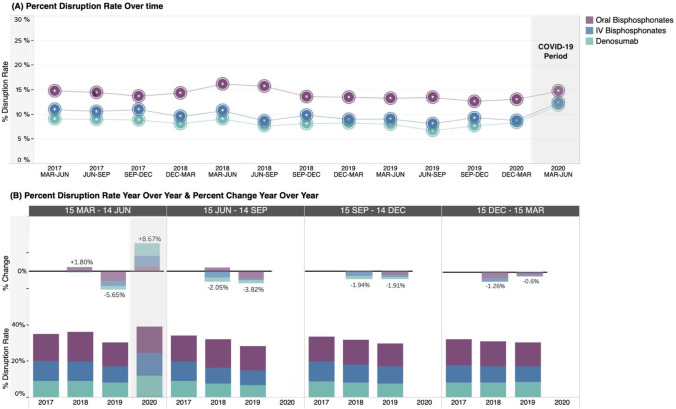
Results: Relative to the average control March to June period, all HCRU declined during the corresponding COVID-19 period. There was a reduction of 14% in patients with osteoporosis healthcare encounters, 13% in general practitioner visits, 9% in specialist practitioner visits, 47% in bone mineral density tests, and 13% in vitamin D tests. Treatment initiations declined 43%, 26%, and 35% for oral bisphosphonates, intravenous bisphosphonates, and denosumab, respectively. Slight increases were observed in the proportion of patients with treatment disruptions. In the subsequent June to September period, HCRU either returned to or surpassed pre-pandemic levels, when including telehealth visits accounting for 33-45% of healthcare encounters during the COVID periods. Oral bisphosphonate treatment initiations remained lower than pre-pandemic levels.
Conclusions: This study demonstrates the COVID-19 pandemic and corresponding public health lockdowns further heightened the "crisis" around the known gap in osteoporosis care and altered the provision of care (e.g., use of telehealth and initiation of treatment). Osteoporosis has a known substantial care and management disparity, which has been classified as a crisis. The COVID-19 pandemic created additional burden on osteoporosis patient care with healthcare encounters, physician visits, diagnostic and laboratory tests, and treatment initiations all declining during the initial pandemic period, relative to previous years.
Keywords: COVID-19; Care patterns; Healthcare resource utilization; Osteoporosis; Pandemic.
© 2022. The Author(s).
Conflict of interest statement
SM, EG, MSF, and SL are employed by Medlior, which received funding for the study from Amgen Canada. TO, RW, MP, and SA are employed by Amgen Canada who funded this study and hold Amgen stock. DLK reports research support from Amgen, Astellas, AstraZeneca, and Eli Lilly, consulting fees from Amgen, Eli Lilly, Merck, and Pfizer, and is on the speakers’ bureau for Amgen, Eli Lilly, and GSK. JPB reports research support from Mereo BioPharma, Radius Health and Servier, consulting fees from Amgen, Paladin Labs Inc., Pfizer, and Servier, and is on the speakers’ bureau for Amgen. AGJ has participated in Advisory Boards for Amgen Canada and Paladin Labs Inc, and is on the speaker bureau for Amgen. PS reports research support from Johnson & Johnson, Smith & Nephew, and DePuy Synthes and has participated on Advisory Boards for Amgen.
Figures
Similar articles
-
Trends in major adverse cardiac events and healthcare utilization during the COVID-19 pandemic in Alberta, Canada.CJC Open. 2023 Jun 22;5(10):719-27. doi: 10.1016/j.cjco.2023.06.004. Online ahead of print. CJC Open. 2023. PMID: 37366514 Free PMC article.
-
Trends in osteoporotic fracture and related in-hospital complications during the COVID-19 pandemic in Alberta, Canada.Arch Osteoporos. 2022 Aug 3;17(1):109. doi: 10.1007/s11657-022-01114-9. Arch Osteoporos. 2022. PMID: 35920903 Free PMC article.
-
Increased Virtual Visits to Physicians During the COVID-19 Pandemic and Estimated Impact on Physician Compensation: The Case of Lung and Colorectal Cancers, Chronic Obstructive Pulmonary Diseases, and Heart Failure in Alberta, Canada.Telemed J E Health. 2024 Jun;30(7):e2024-e2039. doi: 10.1089/tmj.2023.0630. Epub 2024 Apr 24. Telemed J E Health. 2024. PMID: 38656126
-
Challenges and Opportunities for Osteoporosis Care During the COVID-19 Pandemic.J Clin Endocrinol Metab. 2021 Nov 19;106(12):e4795-e4808. doi: 10.1210/clinem/dgab570. J Clin Endocrinol Metab. 2021. PMID: 34343287 Free PMC article. Review.
-
Health Care for All: Undocumented Migrants and the COVID-19 Pandemic in Alberta, Canada-A Scoping Review.J Migr Health. 2023;7:100192. doi: 10.1016/j.jmh.2023.100192. Epub 2023 Jun 8. J Migr Health. 2023. PMID: 37317684 Free PMC article.
Cited by
-
Bad to the bones: prescribing of drugs for the prevention and treatment of osteoporosis in patients on chronic glucocorticoids.Arch Osteoporos. 2023 Mar 1;18(1):38. doi: 10.1007/s11657-023-01222-0. Arch Osteoporos. 2023. PMID: 36856881 Free PMC article.
-
On-time denosumab dosing recovered rapidly during the COVID-19 pandemic, yet remains suboptimal.JBMR Plus. 2024 Apr 9;8(5):ziae027. doi: 10.1093/jbmrpl/ziae027. eCollection 2024 May. JBMR Plus. 2024. PMID: 38623483 Free PMC article.
-
Care patterns and Traditional Chinese Medicine constitution as factors of depression and anxiety in patients with systemic sclerosis: A cross-sectional study during the COVID-19 pandemic.Front Integr Neurosci. 2023 Feb 14;17:1052683. doi: 10.3389/fnint.2023.1052683. eCollection 2023. Front Integr Neurosci. 2023. PMID: 36864895 Free PMC article.
References
-
- Curtis EM, van der Velde R, Moon RJ, van den Bergh JP, Geusens P, de Vries F, van Staa TP, Cooper C, Harvey NC. Epidemiology of fractures in the United Kingdom 1988–2012: Variation with age, sex, geography, ethnicity and socioeconomic status. Bone. 2016;87:19–26. doi: 10.1016/j.bone.2016.03.006. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
