

Survival Benefit of Living-Donor Liver Transplant
- PMID: 35921119
- PMCID: PMC9350845
- DOI: 10.1001/jamasurg.2022.3327
Survival Benefit of Living-Donor Liver Transplant
Abstract
Importance: Despite the acceptance of living-donor liver transplant (LDLT) as a lifesaving procedure for end-stage liver disease, it remains underused in the United States. Quantification of lifetime survival benefit and the Model for End-stage Liver Disease incorporating sodium levels (MELD-Na) score range at which benefit outweighs risk in LDLT is necessary to demonstrate its safety and effectiveness.
Objective: To assess the survival benefit, life-years saved, and the MELD-Na score at which that survival benefit was obtained for individuals who received an LDLT compared with that for individuals who remained on the wait list.
Design, setting, and participants: This case-control study was a retrospective, secondary analysis of the Scientific Registry of Transplant Recipients database of 119 275 US liver transplant candidates and recipients from January 1, 2012, to September 2, 2021. Liver transplant candidates aged 18 years or older who were assigned to the wait list (N = 116 455) or received LDLT (N = 2820) were included. Patients listed for retransplant or multiorgan transplant and those with prior kidney or liver transplants were excluded.
Exposures: Living-donor liver transplant vs remaining on the wait list.
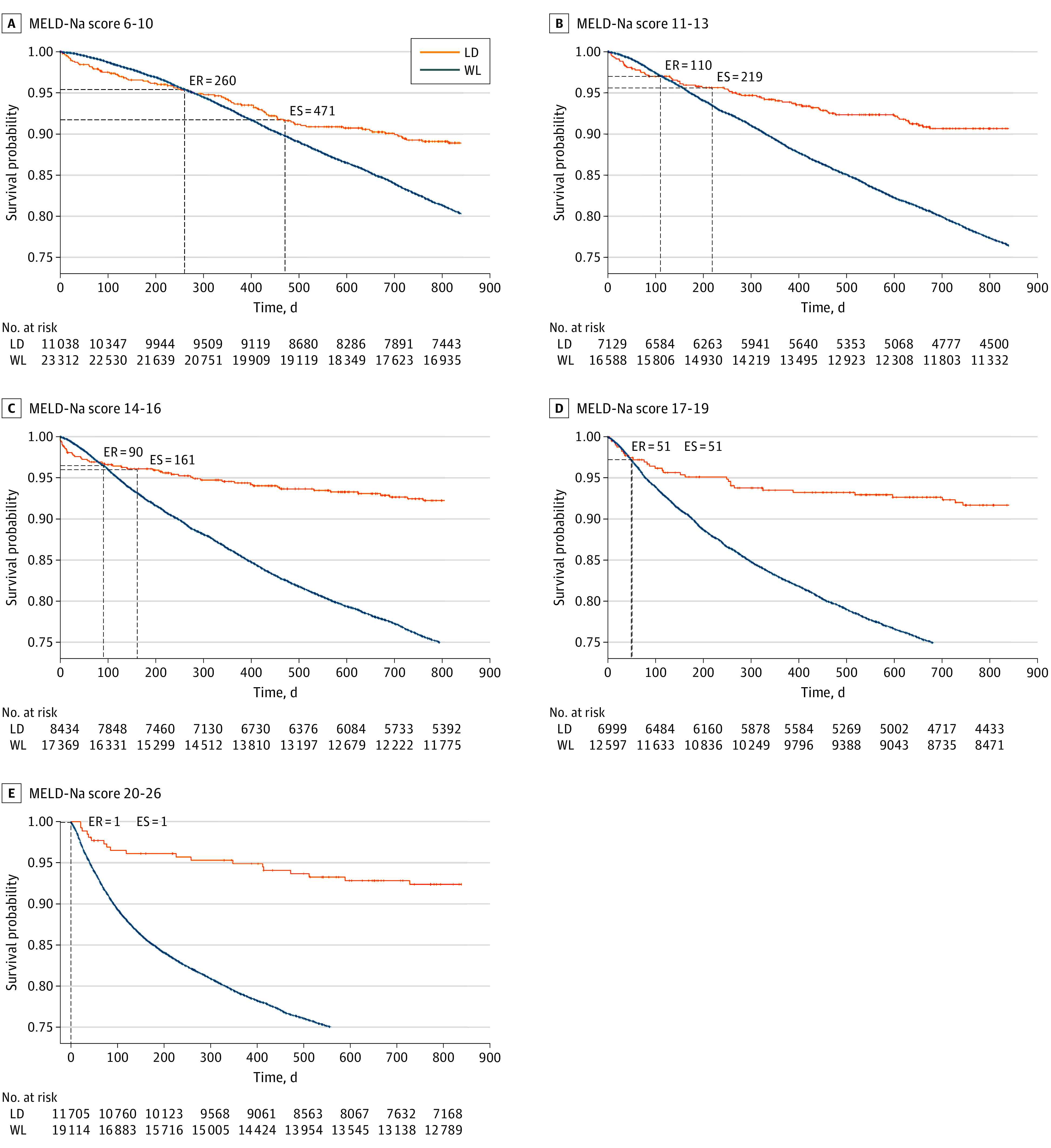
Main outcomes and measures: The primary outcome of this study was life-years saved from receiving an LDLT. Secondary outcomes included 1-year relative mortality and risk, time to equal risk, time to equal survival, and the MELD-Na score at which that survival benefit was obtained for individuals who received an LDLT compared with that for individuals who remained on the wait list. MELD-Na score ranges from 6 to 40 and is well correlated with short-term survival. Higher MELD-Na scores (>20) are associated with an increased risk of death.
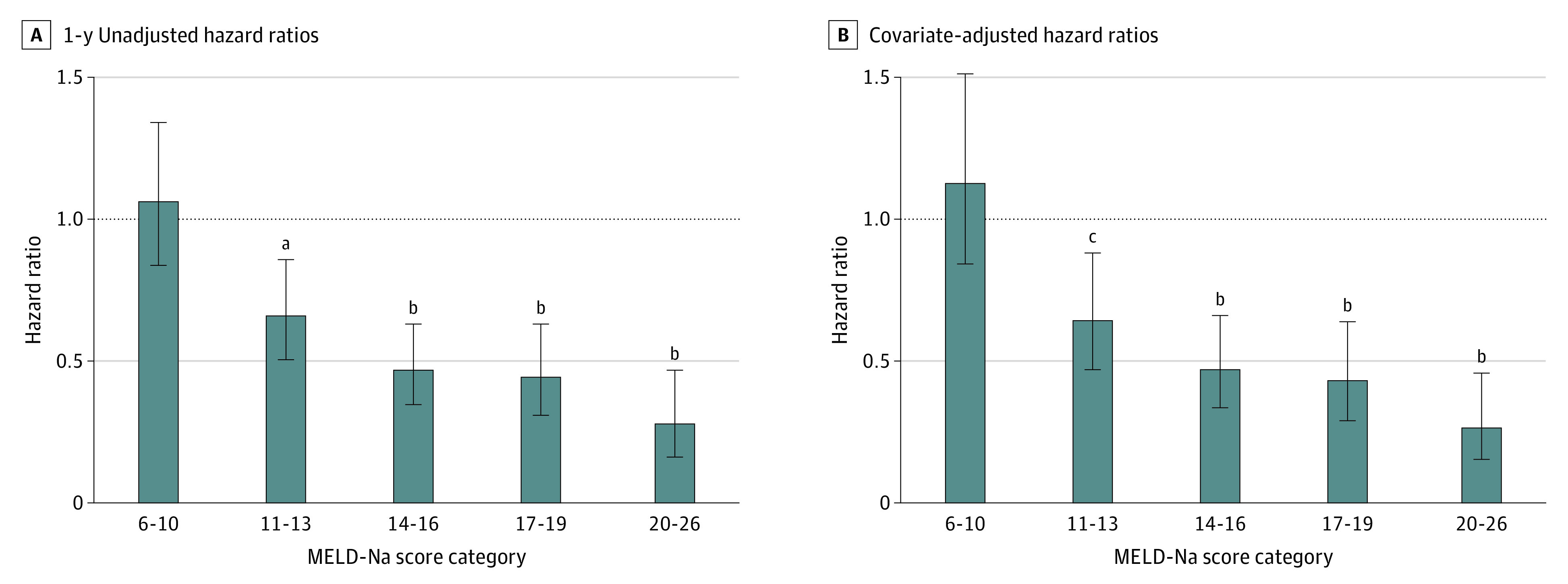
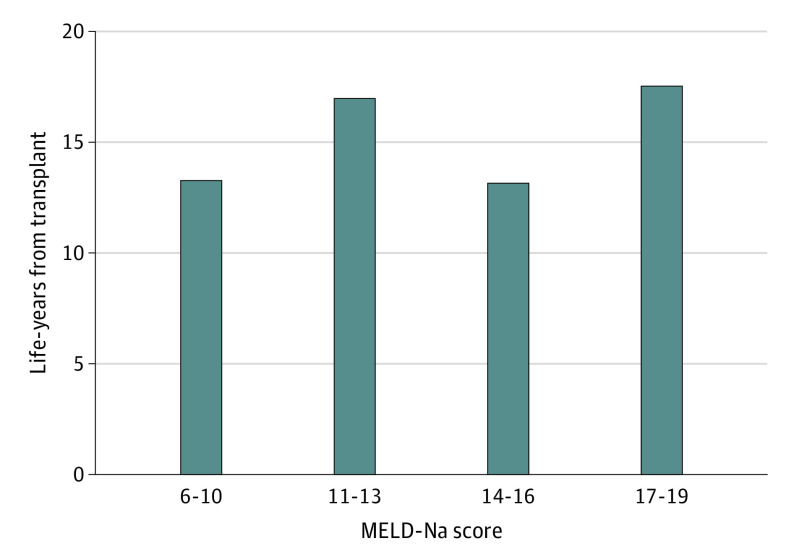
Results: The mean (SD) age of the 119 275 study participants was 55.1 (11.2) years, 63% were male, 0.9% were American Indian or Alaska Native, 4.3% were Asian, 8.2% were Black or African American, 15.8% were Hispanic or Latino, 0.2% were Native Hawaiian or Other Pacific Islander, and 70.2% were White. Mortality risk and survival models confirmed a significant survival benefit for patients receiving an LDLT who had a MELD-Na score of 11 or higher (adjusted hazard ratio, 0.64 [95% CI, 0.47-0.88]; P = .006). Living-donor liver transplant recipients gained an additional 13 to 17 life-years compared with patients who never received an LDLT.
Conclusions and relevance: An LDLT is associated with a substantial survival benefit to patients with end-stage liver disease even at MELD-Na scores as low as 11. The findings of this study suggest that the life-years gained are comparable to or greater than those conferred by any other lifesaving procedure or by a deceased-donor liver transplant. This study's findings challenge current perceptions regarding when LDLT survival benefit occurs.
Conflict of interest statement
Figures
Comment in
-
Just How Low a Model for End-stage Liver Disease Score Benefits From Living-Donor Liver Transplant?JAMA Surg. 2022 Oct 1;157(10):933. doi: 10.1001/jamasurg.2022.3337. JAMA Surg. 2022. PMID: 35921106 No abstract available.
-
A Western World Perspective of Survival Benefit of Living Donor Liver Transplantation: A Commentary to the Article by Jackson et al. Published in JAMA Surgery.Transpl Int. 2022 Oct 25;35:10931. doi: 10.3389/ti.2022.10931. eCollection 2022. Transpl Int. 2022. PMID: 36388426 Free PMC article. No abstract available.
-
Living-Donor Liver Transplant for Patients With End-stage Liver Disease.JAMA Surg. 2023 Apr 1;158(4):427. doi: 10.1001/jamasurg.2022.7000. JAMA Surg. 2023. PMID: 36630123 No abstract available.
-
Living-Donor Liver Transplant for Patients With End-stage Liver Disease.JAMA Surg. 2023 Apr 1;158(4):428. doi: 10.1001/jamasurg.2022.7002. JAMA Surg. 2023. PMID: 36630127 No abstract available.
-
Living-Donor Liver Transplant for Patients With End-stage Liver Disease.JAMA Surg. 2023 Apr 1;158(4):427-428. doi: 10.1001/jamasurg.2022.7001. JAMA Surg. 2023. PMID: 36630132 No abstract available.
-
Living-Donor Liver Transplant for Patients With End-stage Liver Disease-Reply.JAMA Surg. 2023 Apr 1;158(4):428-429. doi: 10.1001/jamasurg.2022.7003. JAMA Surg. 2023. PMID: 36630146 No abstract available.
