

Therapeutic Value of Sentinel Lymph Node Biopsy in Patients With Melanoma: A Randomized Clinical Trial
- PMID: 35921122
- PMCID: PMC9475390
- DOI: 10.1001/jamasurg.2022.2055
Therapeutic Value of Sentinel Lymph Node Biopsy in Patients With Melanoma: A Randomized Clinical Trial
Erratum in
-
Errors in Byline.JAMA Surg. 2022 Sep 1;157(9):859. doi: 10.1001/jamasurg.2022.4558. JAMA Surg. 2022. PMID: 36102914 Free PMC article. No abstract available.
Abstract
Importance: Sentinel lymph node (SLN) biopsy is a standard staging procedure for cutaneous melanoma. Regional disease control is a clinically important therapeutic goal of surgical intervention, including nodal surgery.
Objective: To determine how frequently SLN biopsy without completion lymph node dissection (CLND) results in long-term regional nodal disease control in patients with SLN metastases.
Design, setting, and participants: The second Multicenter Selective Lymphadenectomy Trial (MSLT-II), a prospective multicenter randomized clinical trial, randomized participants with SLN metastases to either CLND or nodal observation. The current analysis examines observation patients with regard to regional nodal recurrence. Trial patients were aged 18 to 75 years with melanoma metastatic to SLN(s). Data were collected from December 2004 to April 2019, and data were analyzed from July 2020 to January 2022.
Interventions: Nodal observation with ultrasonography rather than CLND.
Main outcomes and measures: In-basin nodal recurrence.
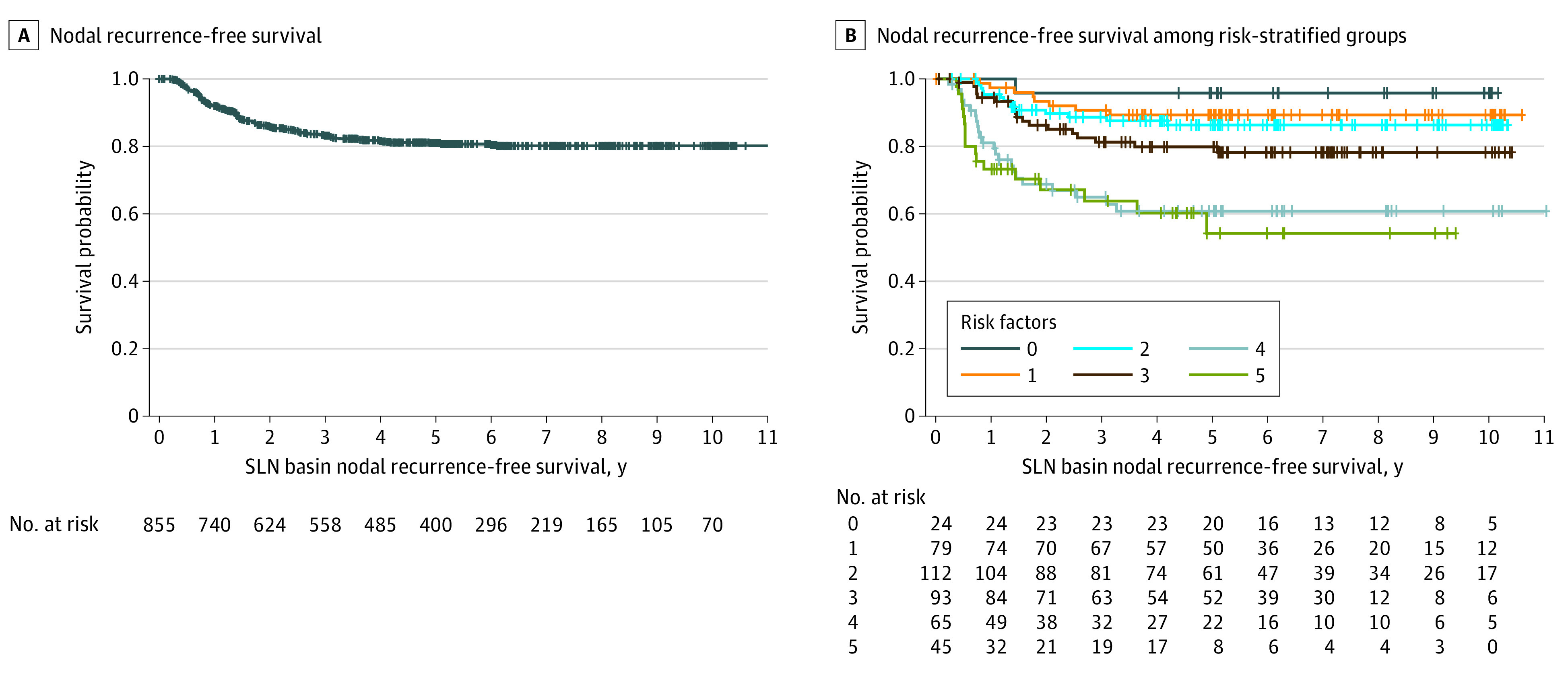
Results: Of 823 included patients, 479 (58.2%) were male, and the mean (SD) age was 52.8 (13.8) years. Among 855 observed basins, at 10 years, 80.2% (actuarial; 95% CI, 77-83) of basins were free of nodal recurrence. By univariable analysis, freedom from regional nodal recurrence was associated with age younger than 50 years (hazard ratio [HR], 0.49; 95% CI, 0.34-0.70; P < .001), nonulcerated melanoma (HR, 0.36; 95% CI, 0.36-0.49; P < .001), thinner primary melanoma (less than 1.5 mm; HR, 0.46; 95% CI, 0.27-0.78; P = .004), axillary basin (HR, 0.61; 95% CI, 0.44-0.86; P = .005), fewer positive SLNs (1 vs 3 or more; HR, 0.32; 95% CI, 0.14-0.75; P = .008), and SLN tumor burden (measured by diameter less than 1 mm [HR, 0.39; 95% CI, 0.26-0.60; P = .001] or less than 5% area [HR, 0.36; 95% CI, 0.24-0.54; P < .001]). By multivariable analysis, younger age (HR, 0.57; 95% CI, 0.39-0.84; P = .004), thinner primary melanoma (HR, 0.40; 95% CI, 0.22-0.70; P = .002), axillary basin (HR, 0.55; 95% CI, 0.31-0.96; P = .03), SLN metastasis diameter less than 1 mm (HR, 0.52; 95% CI, 0.33-0.81; P = .007), and area less than 5% (HR, 0.58; 95% CI, 0.38-0.88; P = .01) were associated with basin control. When looking at the identified risk factors of age (50 years or older), ulceration, Breslow thickness greater than 3.5 mm, nonaxillary basin, and tumor burden of maximum diameter of 1 mm or greater and/or metastasis area of 5% or greater and excluding missing value cases, basin disease-free rates at 5 years were 96% (95% CI, 88-100) for patients with 0 risk factors, 89% (95% CI, 82-96) for 1 risk factor, 86% (95% CI, 80-93) for 2 risk factors, 80% (95% CI, 71-89) for 3 risk factors, 61% (95% CI, 48-74) for 4 risk factors, and 54% (95% CI, 36-72) for 5 or 6 risk factors.
Conclusions and relevance: This randomized clinical trial was the largest prospective evaluation of long-term regional basin control in patients with melanoma who had nodal observation after removal of a positive SLN. SLN biopsy without CLND cleared disease in the affected nodal basin in most patients, even those with multiple risk factors for in-basin recurrence. In addition to its well-validated value in staging, SLN biopsy may also be regarded as therapeutic in some patients.
Trial registration: ClinicalTrials.gov Identifier: NCT00297895.
Conflict of interest statement
Figures
Comment in
-
Prognostic or Therapeutic-The Role of Sentinel Lymph Node Biopsy in Contemporary Practice.JAMA Surg. 2022 Sep 1;157(9):843. doi: 10.1001/jamasurg.2022.2054. JAMA Surg. 2022. PMID: 35921120 No abstract available.
References
-
- Dessureault S, Soong SJ, Ross MI, et al. ; American Joint Committee on Cancer (AJCC) Melanoma Staging Committee . Improved staging of node-negative patients with intermediate to thick melanomas (>1 mm) with the use of lymphatic mapping and sentinel lymph node biopsy. Ann Surg Oncol. 2001;8(10):766-770. doi:10.1007/s10434-001-0766-1 - DOI - PubMed
-
- McMasters KM, Egger ME, Edwards MJ, et al. . Final results of the Sunbelt Melanoma Trial: a multi-institutional prospective randomized phase III study evaluating the role of adjuvant high-dose interferon alfa-2b and completion lymph node dissection for patients staged by sentinel lymph node biopsy. J Clin Oncol. 2016;34(10):1079-1086. doi:10.1200/JCO.2015.63.3776 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
