

The Low Rate of Adherence to Checklist for Artificial Intelligence in Medical Imaging Criteria Among Published Prostate MRI Artificial Intelligence Algorithms
- PMID: 35922018
- PMCID: PMC9887098
- DOI: 10.1016/j.jacr.2022.05.022
The Low Rate of Adherence to Checklist for Artificial Intelligence in Medical Imaging Criteria Among Published Prostate MRI Artificial Intelligence Algorithms
Abstract
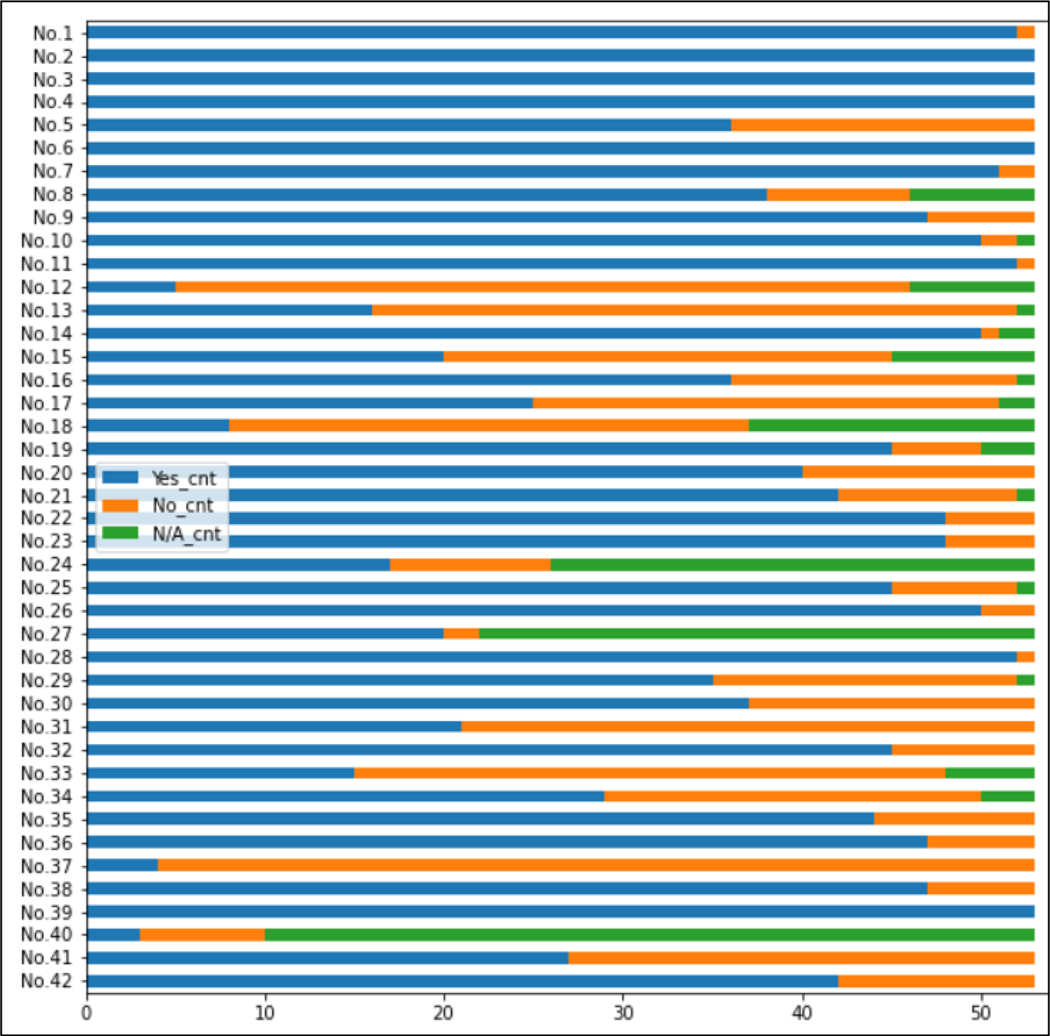
Objective: To determine the rigor, generalizability, and reproducibility of published classification and detection artificial intelligence (AI) models for prostate cancer (PCa) on MRI using the Checklist for Artificial Intelligence in Medical Imaging (CLAIM) guidelines, a 42-item checklist that is considered a measure of best practice for presenting and reviewing medical imaging AI research.
Materials and methods: This review searched English literature for studies proposing PCa AI detection and classification models on MRI. Each study was evaluated with the CLAIM checklist. The additional outcomes for which data were sought included measures of AI model performance (eg, area under the curve [AUC], sensitivity, specificity, free-response operating characteristic curves), training and validation and testing group sample size, AI approach, detection versus classification AI, public data set utilization, MRI sequences used, and definition of gold standard for ground truth. The percentage of CLAIM checklist fulfillment was used to stratify studies into quartiles. Wilcoxon's rank-sum test was used for pair-wise comparisons.
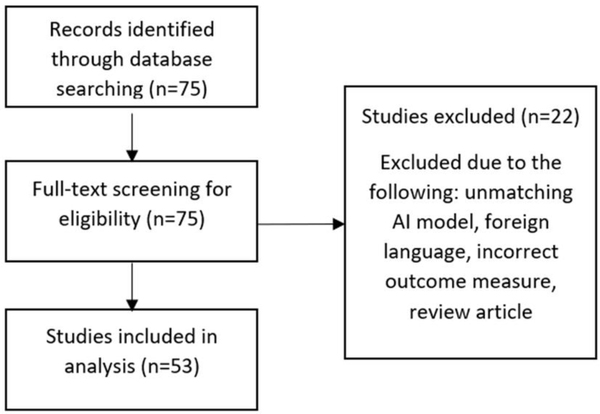
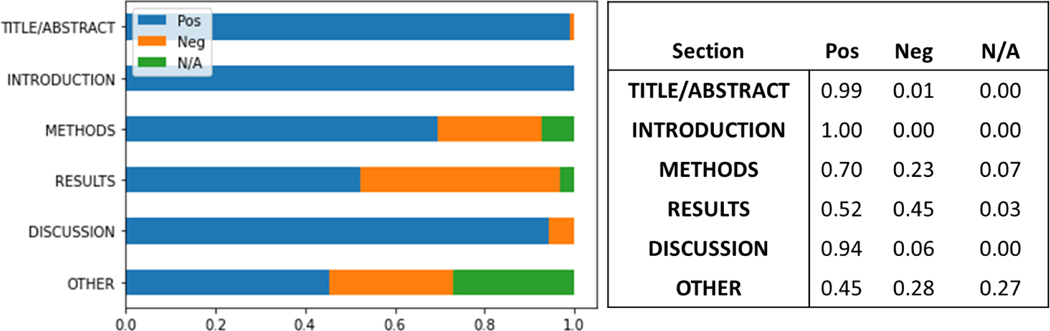
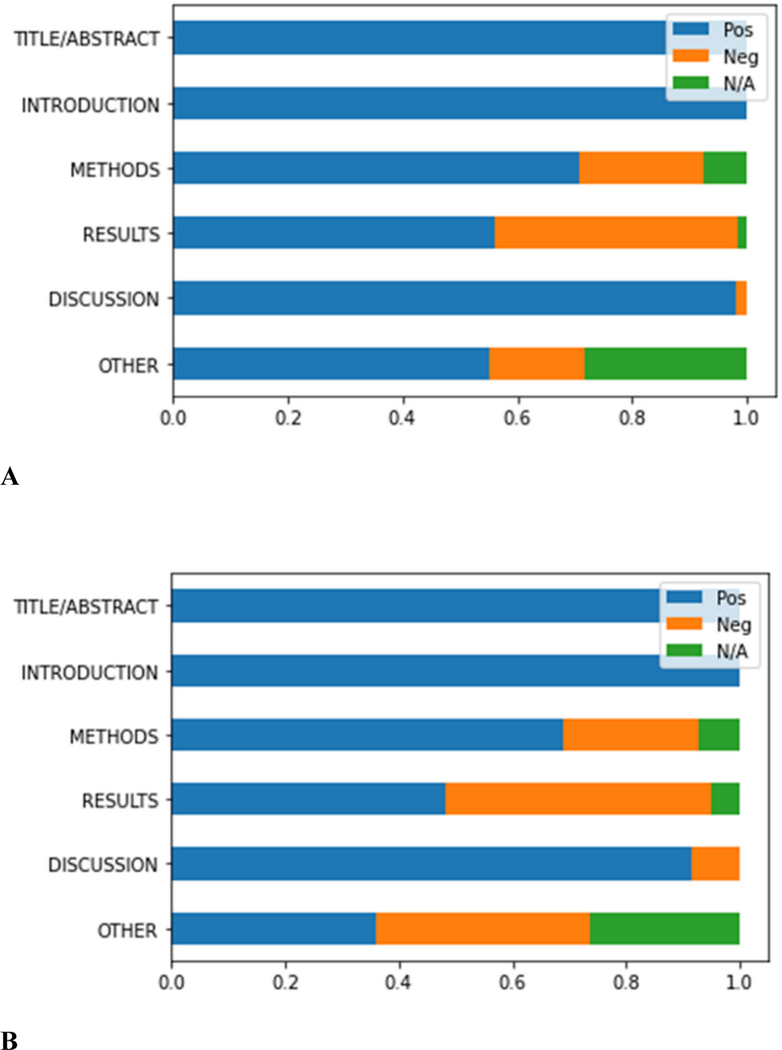
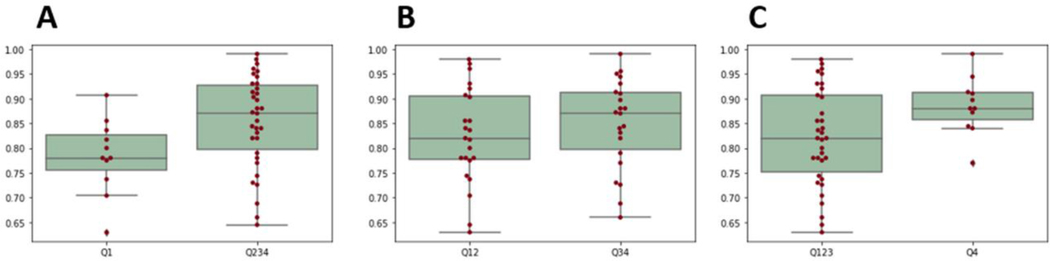
Results: In all, 75 studies were identified, and 53 studies qualified for analysis. The original CLAIM items that most studies did not fulfill includes item 12 (77% no): de-identification methods; item 13 (68% no): handling missing data; item 15 (47% no): rationale for choosing ground truth reference standard; item 18 (55% no): measurements of inter- and intrareader variability; item 31 (60% no): inclusion of validated interpretability maps; item 37 (92% no): inclusion of failure analysis to elucidate AI model weaknesses. An AUC score versus percentage CLAIM fulfillment quartile revealed a significant difference of the mean AUC scores between quartile 1 versus quartile 2 (0.78 versus 0.86, P = .034) and quartile 1 versus quartile 4 (0.78 versus 0.89, P = .003) scores. Based on additional information and outcome metrics gathered in this study, additional measures of best practice are defined. These new items include disclosure of public dataset usage, ground truth definition in comparison to other referenced works in the defined task, and sample size power calculation.
Conclusion: A large proportion of AI studies do not fulfill key items in CLAIM guidelines within their methods and results sections. The percentage of CLAIM checklist fulfillment is weakly associated with improved AI model performance. Additions or supplementations to CLAIM are recommended to improve publishing standards and aid reviewers in determining study rigor.
Keywords: AI; CLAIM; classification; detection; prostate cancer; study rigor.
Published by Elsevier Inc.
Conflict of interest statement
Conflict of Interest
The authors declare no conflict of interest.
Figures
References
-
- Key Statistics for Prostate Cancer | Prostate Cancer Facts [Internet]. Available from: https://www.cancer.org/cancer/prostate-cancer/about/key-statistics.html
-
- Wildeboer RR, van Sloun RJG, Wijkstra H, Mischi M. Artificial intelligence in multiparametric prostate cancer imaging with focus on deep-learning methods. Comput Methods Programs Biomed. 2020. Jun;189:105316. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
