

Distinct immune-effector and metabolic profile of CD8+ T cells in patients with autoimmune polyarthritis induced by therapy with immune checkpoint inhibitors
- PMID: 35922125
- PMCID: PMC9664113
- DOI: 10.1136/ard-2022-222451
Distinct immune-effector and metabolic profile of CD8+ T cells in patients with autoimmune polyarthritis induced by therapy with immune checkpoint inhibitors
Abstract
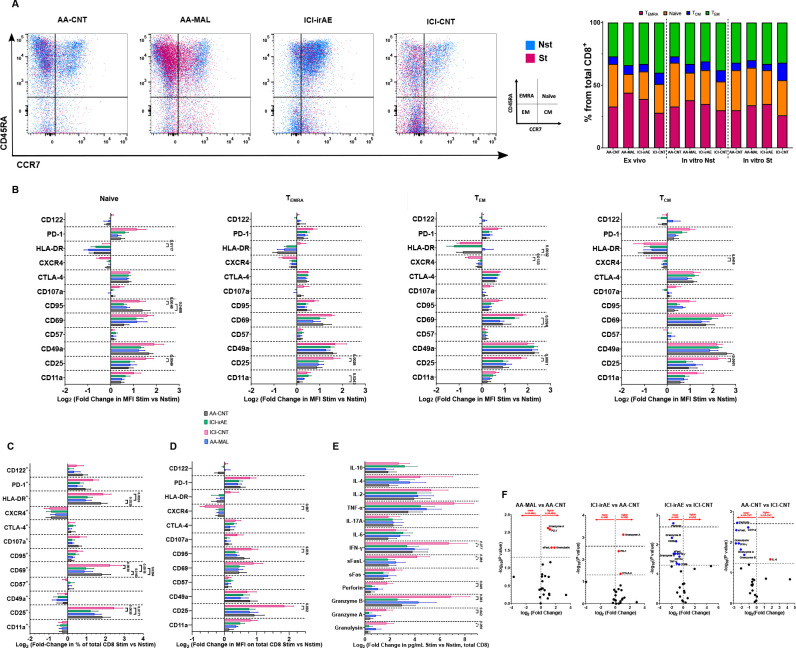
Objectives: Rheumatic immune-related adverse events (irAE) such as (poly)arthritis in patients undergoing immune checkpoint inhibitor (ICI) treatment pose a major clinical challenge. ICI therapy improves CD8+ T cell (CD8) function, but CD8 contributes to chronic inflammation in autoimmune arthritis (AA). Thus, we investigated whether immune functional and metabolic changes in CD8 explain the development of musculoskeletal irAE in ICI-treated patients.
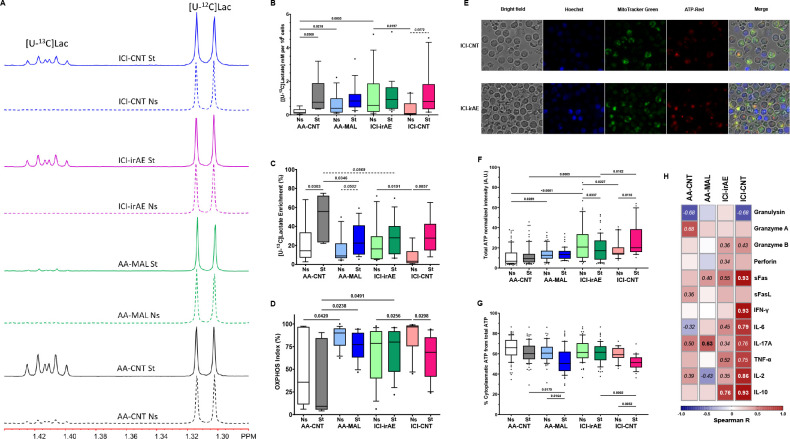
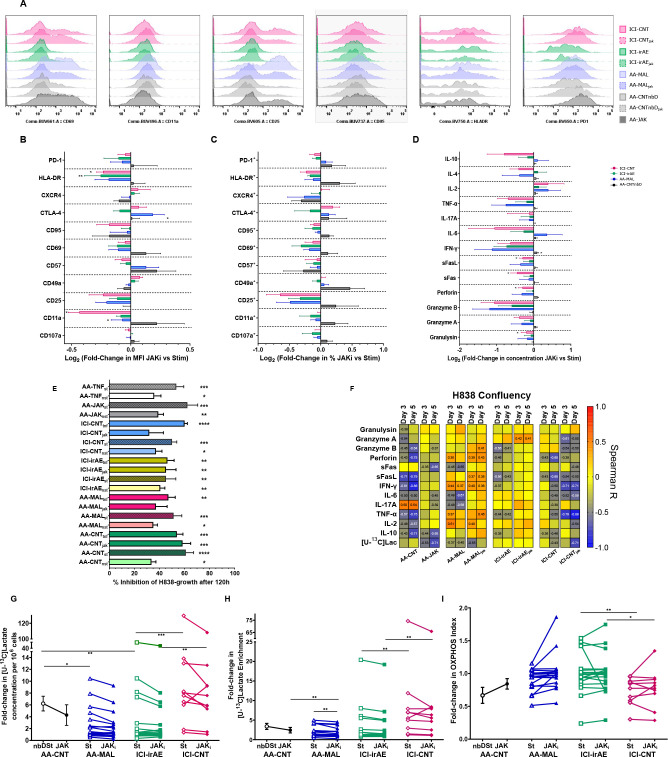
Methods: Peripheral CD8 obtained from ICI-treated patients with and without arthritis irAEs and from AA patients with and without a history of malignancy were stimulated in media containing 13C-labelled glucose with and without tofacitinib or infliximab. Changes in metabolism, immune-mediator release, expression of effector cell-surface molecules and inhibition of tumour cell growth were quantified.
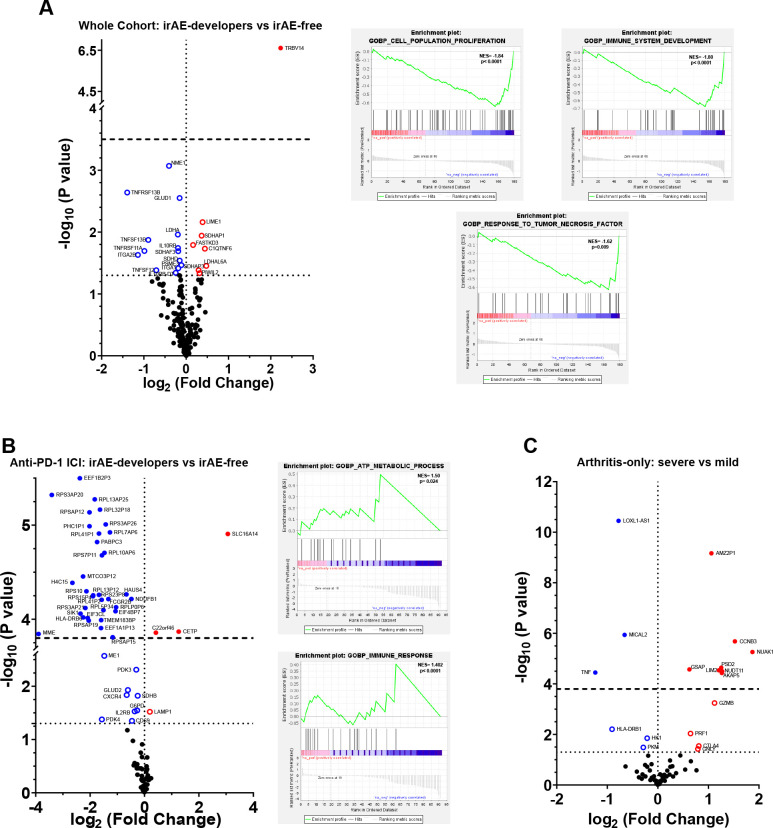
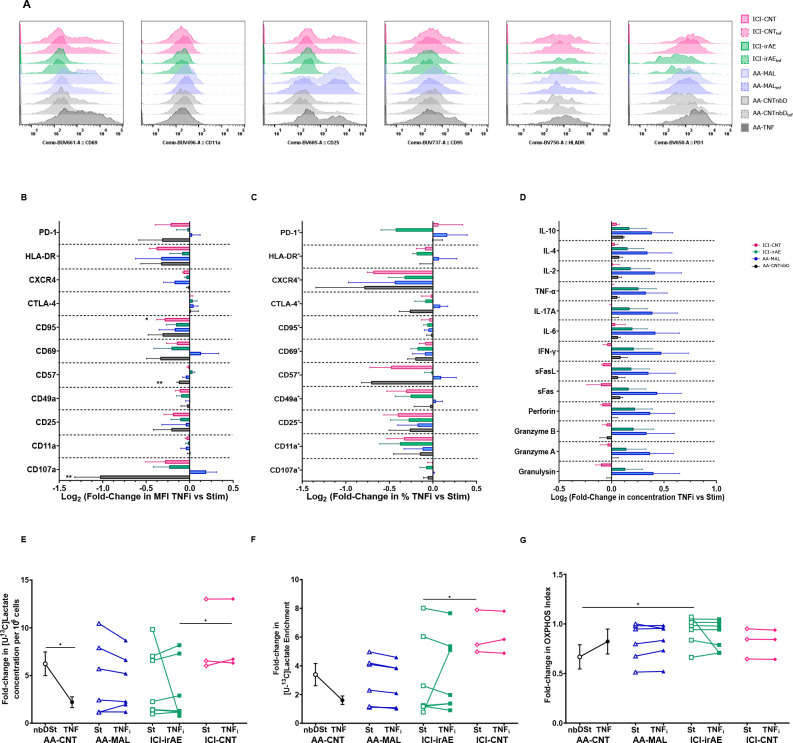
Results: CD8 from patients with irAE showed significantly lower frequency and expression of cell-surface molecule characteristic for activation, effector-functions, homing, exhaustion and apoptosis and reduced release of cytotoxic and proinflammatory immune mediators compared with CD8 from ICI patients who did not develop irAE. This was accompanied by a higher glycolytic rate and ATP production. Gene-expression analysis of pre-ICI-treated CD8 revealed several differentially expressed transcripts in patients who later developed arthritis irAEs. In vitro tofacitinib or infliximab treatment did not significantly change the immune-metabolic profile nor the capacity to release cytolytic mediators that inhibit the growth of the human lung cancer cell line H838.
Conclusions: Our study shows that CD8 from ICI-treated patients who develop a musculoskeletal irAE has a distinct immune-effector and metabolic profile from those that remain irAE free. This specific irAE profile overlaps with the one observed in CD8 from AA patients and may prove useful for novel therapeutic strategies to manage ICI-induced irAEs.
Keywords: Arthritis; Biological Therapy; Inflammation; T-Lymphocyte subsets.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: KB: Consultancy and/or speaker fees and/or travel reimbursements: Abbvie, Bristol Myers Squibb (BMS), Gilead/Galapagos, Janssen, Merck Sharp & Dohme (MSD), Mundipharma, Novartis, Pfizer, Roche, Viatris, UCB. Scientific support: Medical Faculty of University of Heidelberg, Rheumaliga Baden-Württemberg e.V., AbbVie, Novartis. MMSC: Scientific support: Novartis, Pfizer. JCH: honoraria: BMS, MSD, Novartis, Roche, Pierre Fabre, Sanofi, Almirall; consultant or advisory role: MSD, Pierre Fabre, Sunpharma; Scientific support: BMS; Travel support: Pierre Fabre. PC: honoraria: Roche, Takeda, Gilead, AstraZeneca, Novartis; scientific support: Roche, Takeda, Amgen, Merck, AstraZeneca, Novartis; travel support: AstraZeneca, Merck, Janssen, Daiichi Sankyo, Takeda, Novartis, Elli Lilly; data safety monitoring and/or advisory board: Pfizer, Chugai, Boehringer Ingelheim, Roche. JG: honoraria: Galapagos; travel support: Elli Lilly. HML: Scientific funding: Abbvie, Novartis, Pfizer, Roche; consulting fees and honoraria: Abbvie, AstraZeneca, Actelion, Amgen, Bayer Vital, Boehringer Ingelheim, BMS, Celgene, GlaxoSmithKline (GSK), Galapagos, Janssen, Elli Lilly, Medac, MSD, Novartis, Pfizer, Roche, Sanofi, UCB; travel support: Abbvie, AstraZeneca, Boehriner Ingelheim, BMS, Celgene, GSK, Gilead, Janssen, Elli Lilly, MSD, Novartis, Pfizer, Roche, Sanofi, UCB; data safety monitoring and/or advisory board: Abbvie, AstraZeneca, Amgen, Boehriner Ingelheim, BMS, Celgene, GSK, Gilead, Janssen, Elli Lilly, Medac, MSD, Novartis, Pfizer, Roche, Sanofi, UCB
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
