

Antiplatelets Versus Anticoagulation in Cervical Artery Dissection: A Systematic Review and Meta-analysis of 2064 Patients
- PMID: 35922714
- PMCID: PMC9433613
- DOI: 10.1007/s40268-022-00398-z
Antiplatelets Versus Anticoagulation in Cervical Artery Dissection: A Systematic Review and Meta-analysis of 2064 Patients
Abstract
Background and objectives: In young people aged < 50 years, cervical artery dissection (CeAD) is among the most common causes of stroke. Currently, there is no consensus regarding the safest and most effective antithrombotic treatment for CeAD. We aimed to synthesize concrete evidence from studies that compared the efficacy and safety of antiplatelet (AP) versus anticoagulant (AC) therapies for CeAD.
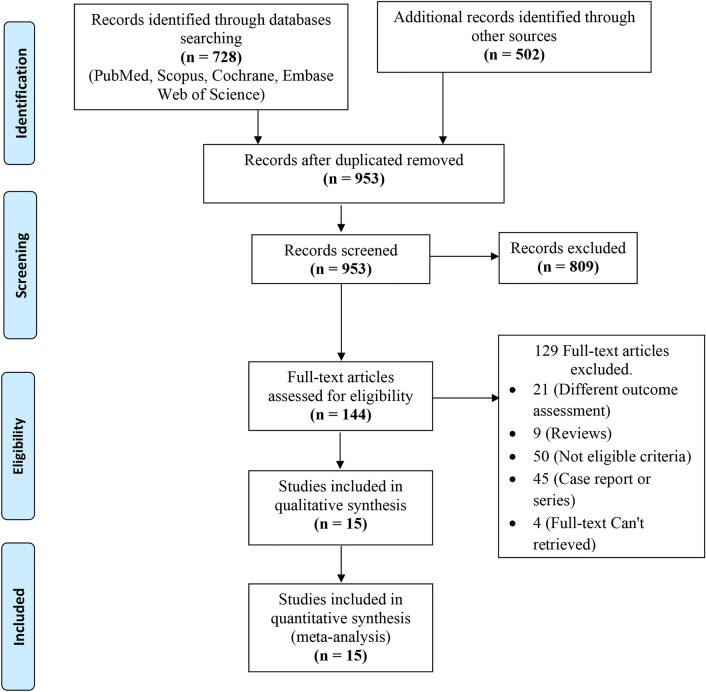
Methods: We searched major electronic databases/search engines from inception till September 2021. Cohort studies and randomized controlled trials (RCTs) comparing anticoagulants with antiplatelets for CeAD were included. A meta-analysis was conducted using articles that were obtained and found to be relevant. Mean difference (MD) with 95% confidence interval (CI) was used for continuous data and odds ratio (OR) with 95% CI for dichotomous data.
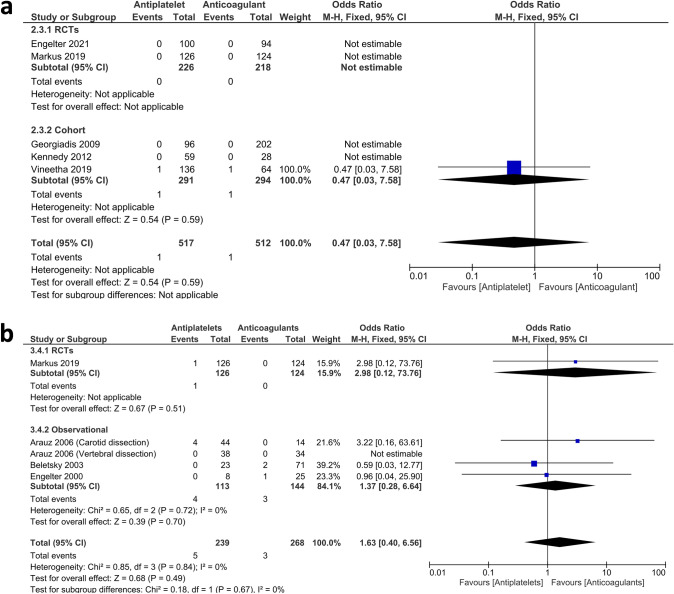
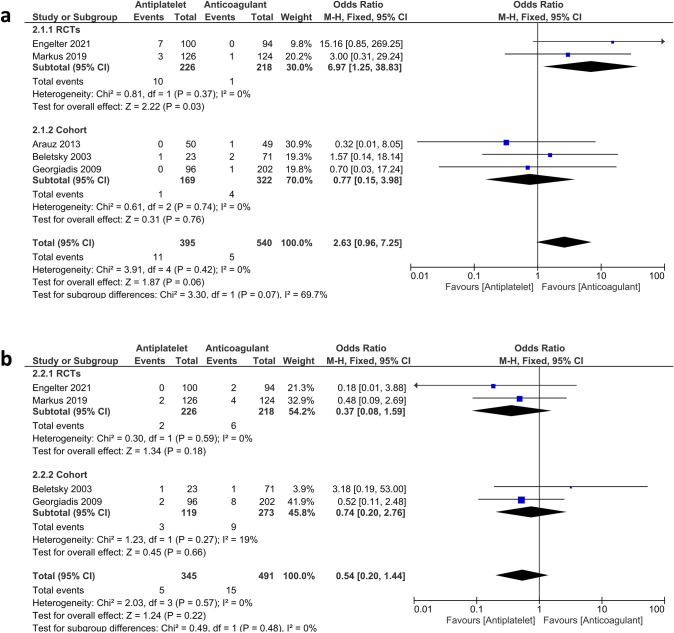
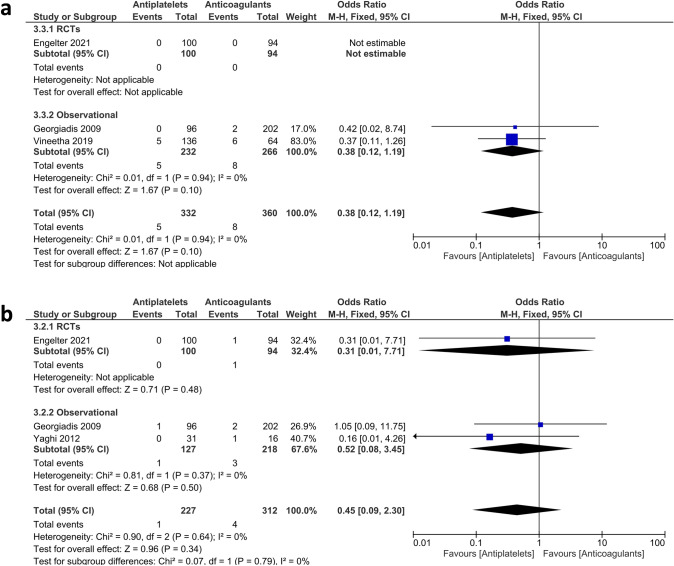
Results: Our analysis included 15 studies involving 2064 patients, 909 (44%) of whom received antiplatelets and 1155 (56%) received anticoagulants. Our analysis showed a non-significant difference in terms of the 3-month mortality (OR 0.47, 95% CI 0.03-7.58), > 3-month mortality (OR 1.63, 95% CI 0.40-6.56), recurrent stroke (OR 0.97, 95% CI 0.46-2.02), recurrent transient ischaemic attack (TIA) (OR 0.93, 95% CI 0.44-1.98), symptomatic intracranial haemorrhage (sICH) (OR 0.38, 95% CI 0.12-1.19), and complete recanalization (OR 0.70, 95% CI 0.46-1.06). Regarding primary ischaemic stroke, the results favoured AC over AP among RCTs (OR 6.97, 95% CI 1.25-38.83).
Conclusion: Our study did not show a considerable difference between the two groups, as all outcomes showed non-significant differences between them, except for primary ischaemic stroke (RCTs) and complete recanalization (observational studies), which showed a significant favour of AC over AP. Even though primary ischaemic stroke is an important outcome, several crucial points that could affect these results should be paid attention to. These include the incomplete adjustment for the confounding effect of AP-AC doses, frequencies, administration compliance, and others. We recommend more well-designed studies to assess if unnecessary anticoagulation can be avoided in CeAD.
© 2022. The Author(s).
Conflict of interest statement
Abdulrahman Ibrahim Hagrass, Bashar Khaled Almaghary, Mohamed Abdelhady Mostafa, Mohamed Elfil, Sarah Makram Elsayed, Amira A. Aboali, Aboalmagd Hamdallah, Mohammed Tarek Hasan, Mohammed Al-kafarna, Khaled Mohamed Ragab and Mohamed Fahmy Doheim declare that they have no potential conflicts of interest that might be relevant to the content of this article.
Figures


Similar articles
-
Antithrombotic Treatment for Cervical Artery Dissection: A Systematic Review and Individual Patient Data Meta-Analysis.JAMA Neurol. 2024 Jun 1;81(6):630-637. doi: 10.1001/jamaneurol.2024.1141. JAMA Neurol. 2024. PMID: 38739383 Free PMC article.
-
Early Anticoagulation or Antiplatelet Therapy Is Critical in Craniocervical Artery Dissection: Results from the COMPASS Registry.Cerebrovasc Dis. 2020;49(4):369-374. doi: 10.1159/000509415. Epub 2020 Jul 30. Cerebrovasc Dis. 2020. PMID: 32731249
-
Antiplatelet treatment compared with anticoagulation treatment for cervical artery dissection (CADISS): a randomised trial.Lancet Neurol. 2015 Apr;14(4):361-7. doi: 10.1016/S1474-4422(15)70018-9. Epub 2015 Feb 12. Lancet Neurol. 2015. PMID: 25684164 Clinical Trial.
-
Preoperative antithrombotic treatment in acutely symptomatic carotid artery stenosis.J Stroke Cerebrovasc Dis. 2022 May;31(5):106396. doi: 10.1016/j.jstrokecerebrovasdis.2022.106396. Epub 2022 Feb 24. J Stroke Cerebrovasc Dis. 2022. PMID: 35219972
-
Anticoagulants or antiplatelets for secondary prevention of cryptogenic stroke: an updated systematic review and meta-analysis.Heart. 2025 May 12;111(11):495-505. doi: 10.1136/heartjnl-2024-325288. Heart. 2025. PMID: 39915077 Free PMC article.
Cited by
-
Microembolic signal detection in acute ischemic stroke: Clinical relevance and impact on treatment individualization-A narrative review.Eur J Neurol. 2025 Jan;32(1):e16584. doi: 10.1111/ene.16584. Eur J Neurol. 2025. PMID: 39706201 Free PMC article. Review.
-
Analysis of differentially expressed genes related to cerebral ischaemia in young rats based on the Gene Expression Omnibus database.World J Clin Cases. 2023 Mar 6;11(7):1467-1476. doi: 10.12998/wjcc.v11.i7.1467. World J Clin Cases. 2023. PMID: 36926408 Free PMC article.
-
Posterior Inferior Cerebellar Artery Stroke Due to a Severe Right Vertebral Artery Stenosis With a Left Cervical Internal Carotid Artery Dissection: What's Next?Cureus. 2024 Mar 5;16(3):e55598. doi: 10.7759/cureus.55598. eCollection 2024 Mar. Cureus. 2024. PMID: 38586807 Free PMC article.
-
Initial clinical experience with Xpert-Pro peripheral self-expanding stent system for internal carotid artery dissection: Two case reports.J Interv Med. 2023 Apr 24;6(2):103-106. doi: 10.1016/j.jimed.2023.04.003. eCollection 2023 May. J Interv Med. 2023. PMID: 37409062 Free PMC article.
References
-
- Fawaz Al MNK, Nitesh D, Rolla N, Raghav G, Naif MA, Ahmed AL, Mohammad El G, Irwin AK, Steven S, Gaurav G, Sudipta R. Updates in the management of cerebral infarctions and subarachnoid hemorrhage secondary to intracranial arterial dissection: a systematic review. World Neurosurg. 2019;121:51–58. doi: 10.1016/j.wneu.2018.09.153. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
