

Le Cœur en Sabot: shape associations with adverse events in repaired tetralogy of Fallot
- PMID: 35922806
- PMCID: PMC9351245
- DOI: 10.1186/s12968-022-00877-x
Le Cœur en Sabot: shape associations with adverse events in repaired tetralogy of Fallot
Abstract
Background: Maladaptive remodelling mechanisms occur in patients with repaired tetralogy of Fallot (rToF) resulting in a cycle of metabolic and structural changes. Biventricular shape analysis may indicate mechanisms associated with adverse events independent of pulmonary regurgitant volume index (PRVI). We aimed to determine novel remodelling patterns associated with adverse events in patients with rToF using shape and function analysis.
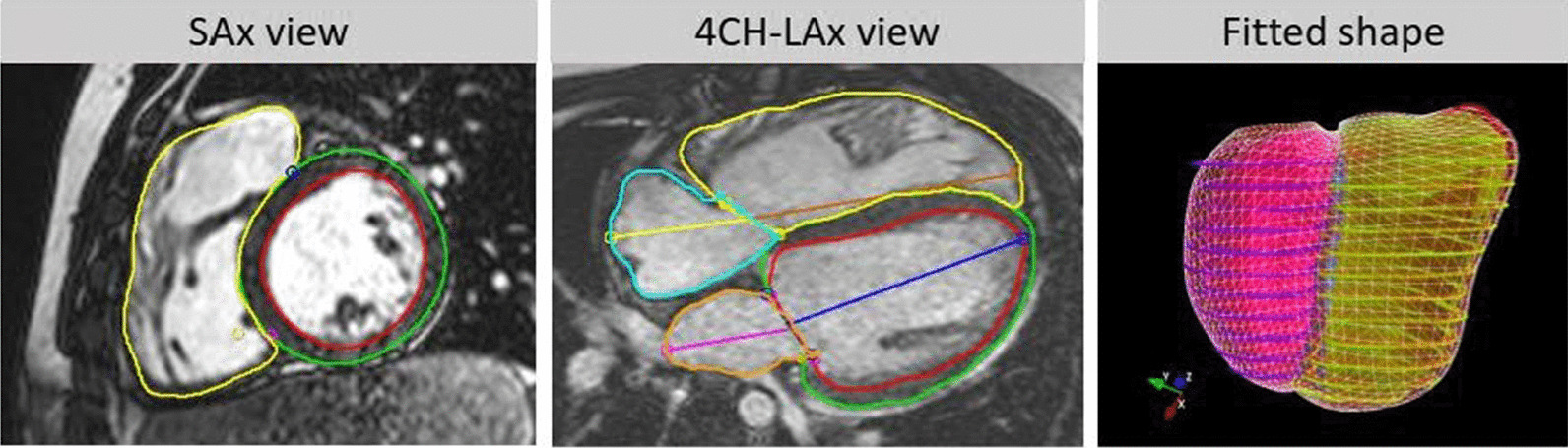
Methods: Biventricular shape and function were studied in 192 patients with rToF (median time from TOF repair to baseline evaluation 13.5 years). Linear discriminant analysis (LDA) and principal component analysis (PCA) were used to identify shape differences between patients with and without adverse events. Adverse events included death, arrhythmias, and cardiac arrest with median follow-up of 10 years.
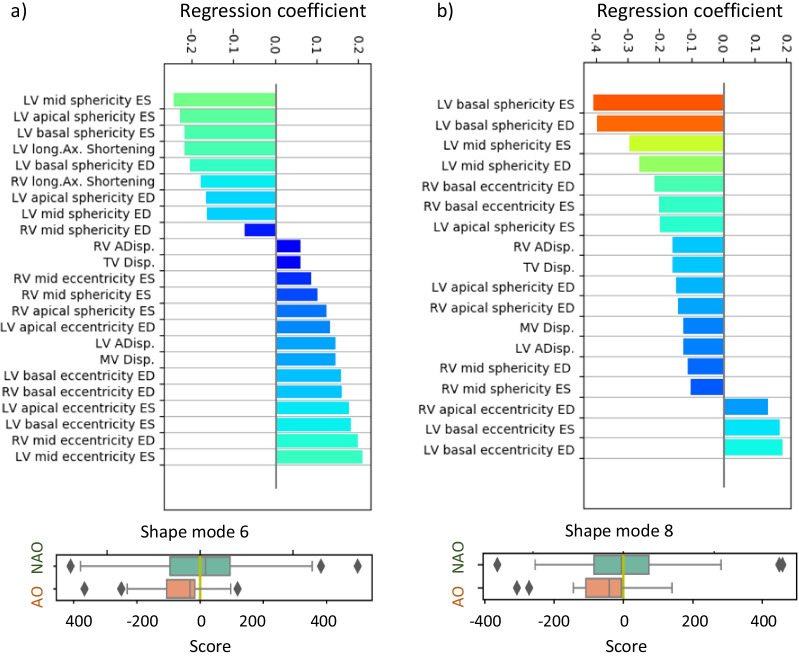
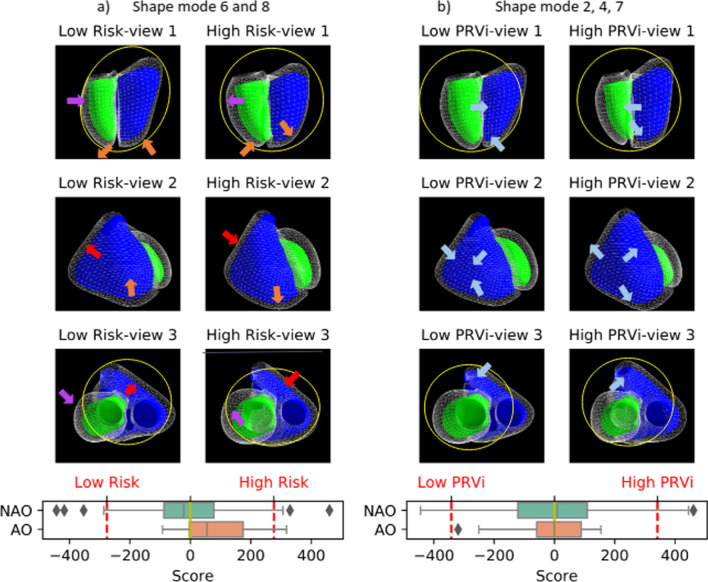
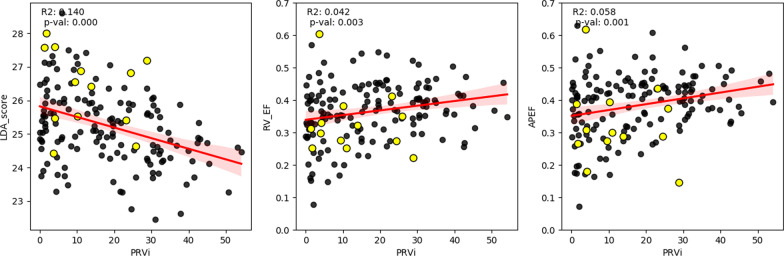
Results: LDA and PCA showed that shape characteristics pertaining to adverse events included a more circular left ventricle (LV) (decreased eccentricity), dilated (increased sphericity) LV base, increased right ventricular (RV) apical sphericity, and decreased RV basal sphericity. Multivariate LDA showed that the optimal discriminative model included only RV apical ejection fraction and one PCA mode associated with a more circular and dilated LV base (AUC = 0.77). PRVI did not add value, and shape changes associated with increased PRVI were not predictive of adverse outcomes.
Conclusion: Pathological remodelling patterns in patients with rToF are significantly associated with adverse events, independent of PRVI. Mechanisms related to incident events include LV basal dilation with a reduced RV apical ejection fraction.
Keywords: Biomarker; Biventricular shape; Magnetic resonance imaging; Tetralogy of Fallot.
© 2022. The Author(s).
Conflict of interest statement
A.D.M. and J.H.O. are co-founders of and have an equity interest in Insilicomed, and A.D.M. has an equity interest in Vektor Medical. A.D.M. and J.H.O. serve on the scientific advisory board of Insilicomed, and A.D.M. as scientific advisor to both companies. Some of their research grants have been identified for conflict of interest management based on the overall scope of the project and its potential benefit to these companies. The authors are required to disclose this relationship in publications acknowledging the grant support; however, the research subject and findings reported in this study did not involve the companies in any way and have no specific relationship with the business activities or scientific interests of either company. The terms of this arrangement have been reviewed and approved by the University of California San Diego in accordance with its conflict of interest policies.
Figures
References
-
- Valente AM, Gauvreau K, Assenza GE, Babu-Narayan SV, Schreier J, Gatzoulis MA, Groenink M, Inuzuka R, Kilner PJ, Koyak Z, et al. Contemporary predictors of death and sustained ventricular tachycardia in patients with repaired tetralogy of Fallot enrolled in the INDICATOR cohort. Heart. 2014;100(3):247–253. doi: 10.1136/heartjnl-2013-304958. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
