

Post-exposure prophylaxis with sotrovimab for Omicron (B.1.1.529) SARS-CoV-2 variant during the aplastic phase of autologous stem cell transplantation
- PMID: 35922822
- PMCID: PMC9351203
- DOI: 10.1186/s13027-022-00454-y
Post-exposure prophylaxis with sotrovimab for Omicron (B.1.1.529) SARS-CoV-2 variant during the aplastic phase of autologous stem cell transplantation
Abstract
Background: To date, there is no information on the safety and efficacy of the novel anti-sarbecoviruses monoclonal antibody sotrovimab administered, as a post-exposure prophylactic measure, during the aplastic phase of autologous stem cell transplantation (ASCT).
Methods: We describe the outcomes of a Multiple Myeloma (MM) patient, who was threateningly exposed to the Omicron (B.1.1.529) SARS-CoV-2 variant, two days after having received a myeloablative regimen of high-dose melphalan. The patient fulfilled all CDC criteria for prolonged close contacts with an index patient who tested positive for a molecular nasopharyngeal swab (Omicron; B.1.1.529) soon after admission to the ward. Given the high risks of morbidity and mortality in the case of COVID-19 developing during the aplastic phase of transplantation, we adopted a post-exposure prophylaxis intervention based on intravenous (i.v.) sotrovimab.
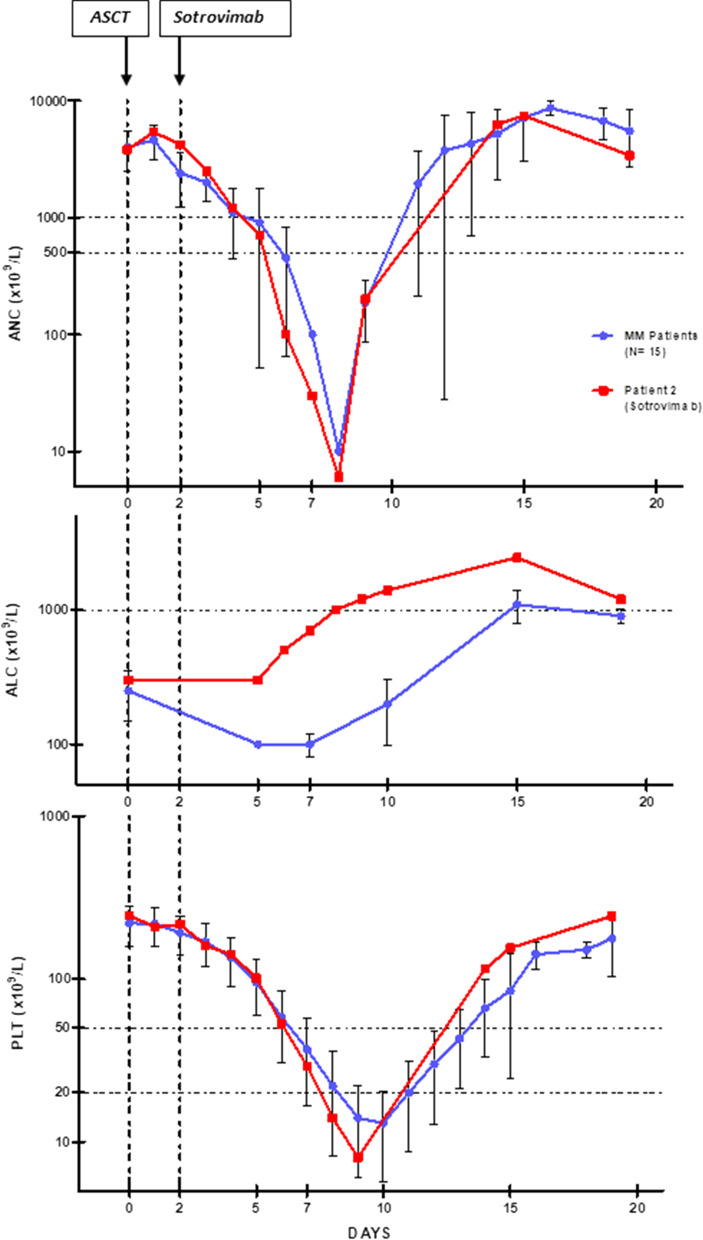
Results: Sotrovimab (500 mg i.v.) was administered at day + 2 from stem cells reinfusion, i.e. 4 days after myeloablative chemotherapy, and at day + 5 from the last close contact with the Omicron-positive index case. The patient was fully protected from SARS-CoV-2 infection throughout his clinical course and remained molecularly negative at the day + 30 from the transplant. We compared times to engraftment and transplant-related toxicities of the sotrovimab-treated patient with the last 15 MM patients transplanted at our Centre, evidencing no unexpected safety signals, infusion-related reactions, or alarming effects on engraftment kinetics.
Conclusions: We have shown here for the first time that administration of sotrovimab during the pre-engraftment phase of ASCT is effective, safe, and not associated with delays in hemopoietic recovery. As compared to MM patients who received the same myeloablative conditioning regimen, the patient given sotrovimab during the aplastic phase did not show any significant differences in engraftment kinetics and toxicity outcomes. Post-exposure prophylaxis with sotrovimab may represent a valuable approach in the stem cell transplantation setting for patients with high-risk exposure to a confirmed COVID-19 case sustained by highly infectious SARS-CoV-2 variants escaping the vaccine-derived immunity due to antigenic shifts in the spike proteins.
Keywords: Autologous stem cell transplantation; Multiple myeloma; SARS-CoV-2 Omicron variant; Sotrovimab.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous
