

This is a preprint.
Health impacts of COVID-19 disruptions to primary cervical screening by time since last screen: A model-based analysis for current and future disruptions
- PMID: 35923317
- PMCID: PMC9347288
- DOI: 10.1101/2022.07.25.22278011
Health impacts of COVID-19 disruptions to primary cervical screening by time since last screen: A model-based analysis for current and future disruptions
Update in
-
A model-based analysis of the health impacts of COVID-19 disruptions to primary cervical screening by time since last screen for current and future disruptions.Elife. 2022 Oct 12;11:e81711. doi: 10.7554/eLife.81711. Elife. 2022. PMID: 36222673 Free PMC article.
Abstract
Background: We evaluated how temporary disruptions to primary cervical cancer (CC) screening services may differentially impact women due to heterogeneity in their screening history and test modality.
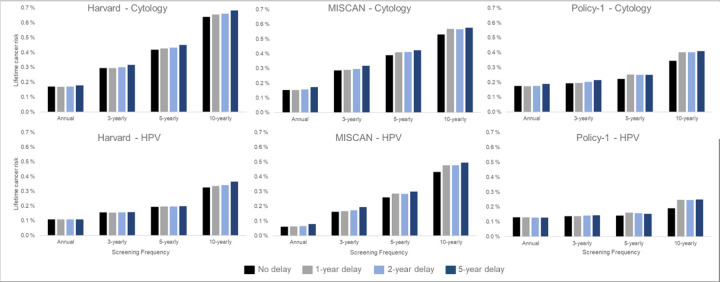
Methods: We used three CC models to project the short- and long-term health impacts assuming an underlying primary screening frequency (i.e., 1, 3, 5, or 10 yearly) under three alternative COVID-19-related screening disruption scenarios (i.e., 1-, 2- or 5-year delay) versus no delay, in the context of both cytology-based and HPV-based screening.
Results: Models projected a relative increase in symptomatically-detected cancer cases during a 1-year delay period that was 38% higher (Policy1-Cervix), 80% higher (Harvard) and 170% higher (MISCAN-Cervix) for under-screened women whose last cytology screen was 5 years prior to the disruption period compared with guidelines-compliant women (i.e., last screen three years prior to disruption). Over a woman's lifetime, temporary COVID-19-related delays had less impact on lifetime risk of developing CC than screening frequency and test modality; however, CC risks increased disproportionately the longer time had elapsed since a woman's last screen at the time of the disruption. Excess risks for a given delay period were generally lower for HPV-based screeners than for cytology-based screeners.
Conclusions: Our independent models predicted that the main drivers of CC risk were screening frequency and screening modality, and the overall impact of disruptions from the pandemic on CC outcomes may be small. However, screening disruptions disproportionately affect under-screened women, underpinning the importance of reaching such women as a critical area of focus, regardless of temporary disruptions.
Funding: This study was supported by funding from the National Cancer Institute (U01CA199334). The contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Cancer Institute. Megan A Smith receives salary support from the National Health and Medical Research Council, Australia (APP1159491) and Cancer Institute NSW (ECF181561). Matejka Rebolj is funded by Cancer Research UK (reference: C8162/A27047). James O'Mahony is funded by Ireland's Health Research Board (EIA2017054). Karen Canfell receives salary support from the National Health and Medical Research Council, Australia (APP1194679). Emily A. Burger receives salary support from the Norwegian Cancer Society.
Conflict of interest statement
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Karen Canfell is the co-PI of an investigator-initiated trial of CC screening, Compass, run by the VCS Foundation, which is a government-funded not-for-profit charity. Neither KC nor her institution have received funding from industry for this or any other research project. All other authors declare no conflicts. Emily A Burger receives salary support from the Norwegian Cancer Society (#198073), and Megan A Smith receives salary support from the National Health and Medical Research Council, Australia (APP1159491) and Cancer Institute NSW (ECF181561). Matejka Rebolji: Public Health England provided funding for evaluation of various PHE projects; member of various PHE advisory groups for cervical screening; attended meetings with various HPV assay manufacturers; fee for lecture in the last four years from Hologic, paid to employer.
Figures




Similar articles
-
A model-based analysis of the health impacts of COVID-19 disruptions to primary cervical screening by time since last screen for current and future disruptions.Elife. 2022 Oct 12;11:e81711. doi: 10.7554/eLife.81711. Elife. 2022. PMID: 36222673 Free PMC article.
-
Impact of COVID-19-related care disruptions on cervical cancer screening in the United States.J Med Screen. 2021 Jun;28(2):213-216. doi: 10.1177/09691413211001097. Epub 2021 Mar 17. J Med Screen. 2021. PMID: 33730899 Free PMC article.
-
Impact of the COVID-19 pandemic on faecal immunochemical test-based colorectal cancer screening programmes in Australia, Canada, and the Netherlands: a comparative modelling study.Lancet Gastroenterol Hepatol. 2021 Apr;6(4):304-314. doi: 10.1016/S2468-1253(21)00003-0. Epub 2021 Feb 3. Lancet Gastroenterol Hepatol. 2021. PMID: 33548185 Free PMC article.
-
Guidelines for Cervical Cancer Screening in Immunosuppressed Women Without HIV Infection.J Low Genit Tract Dis. 2019 Apr;23(2):87-101. doi: 10.1097/LGT.0000000000000468. J Low Genit Tract Dis. 2019. PMID: 30907775
-
Screening for Cervical Cancer With High-Risk Human Papillomavirus Testing: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Aug. Report No.: 17-05231-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 Aug. Report No.: 17-05231-EF-1. PMID: 30256575 Free Books & Documents. Review.
References
-
- Fisher-Borne M, Isher-Witt J, Comstock S, Perkins RB. Understanding COVID-19 impact on cervical, breast, and colorectal cancer screening among federally qualified healthcare centers participating in “Back on track with screening” quality improvement projects. Prev Med. 2021;151:106681. - PMC - PubMed
-
- Mast C, Munoz del Rio A. Delayed cancer screenings—a second look. Verona, WI: Epic Health Research Network; 2020. https://ehrn.org/articles/delayed-cancer-screenings-a-second-lookexternal Accessed February 5, 2021.
-
- Epic Research. “Troubling Cancer Screening Rates Still Seen Nearly Two Years Into the Pandemic.” Accessed May 5, 2022. Available at: https://epicresearch.org/articles/troubling-cancer-screening-rates-still... [
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources