

The role of social risk factors and engagement with maternity services in ethnic disparities in maternal mortality: A retrospective case note review
- PMID: 35923429
- PMCID: PMC9340503
- DOI: 10.1016/j.eclinm.2022.101587
The role of social risk factors and engagement with maternity services in ethnic disparities in maternal mortality: A retrospective case note review
Abstract
Background: Reasons for ethnic disparities in maternal death in the UK are unclear and may be explained by differences in social risk factors and engagement with maternity services.
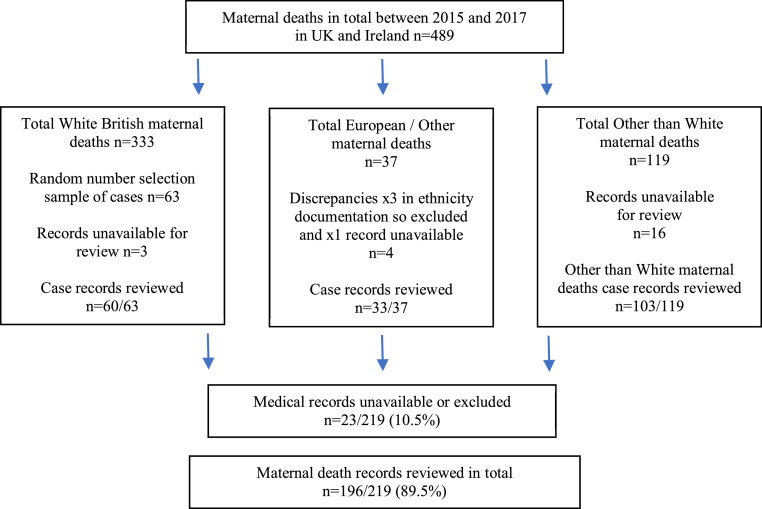
Methods: In this retrospective systematic case note review, we used anonymised medical records from MBRRACE-UK for all Other than White, and White European/Other women plus a random sample of White British/Irish women who died in pregnancy or up to 1 year afterwards from 01/01/2015 to 12/31/2017. We used a standardised data extraction tool developed from a scoping review to explore social risk factors and engagement with maternity services.
Findings: Of 489 women identified, 219 were eligible for the study and 196 case notes were reviewed, including 103/119 from Other than White groups, 33/37 White European/Other and a random sample of 60/333 White British/Irish. The presence of three or more social risk factors was 11⋅7% (12/103) in Other than White women, 18⋅2% (6/33) for White European/Other women and 36⋅7% (22/60) in White British/Irish women. Across all groups engagement with maternity services was good with 85⋅5% (148/196) receiving the recommended number of antenatal appointments as was completion of antenatal mental health assessment (123/173, 71⋅1%). 15⋅5% (16/103) of Other than White groups had pre-existing co-morbidities and 51⋅1% (47/92) had previous pregnancy problems while women across White ethnic groups had 3⋅2% (3/93) and 33⋅3% (27/81) respectively. Three or more unscheduled healthcare attendances occurred in 60⋅0% (36/60) of White British/Irish, 39⋅4% (13/33) in White European/Other and 35⋅9% (37/103) of Other than White women. Evidence of barriers to following healthcare advice was identified for a fifth of all women. None of the 17 women who required an interpreter received appropriate provision at all key points throughout their maternity care.
Interpretation: Neither increased social risk factors or barriers to engagement with maternity services appear to underlie disparities in maternal mortality. Management of complex social factors and interpreter services need improvement.
Funding: National Institute for Health Research (NIHR) Applied Research Collaboration West Midlands.
Keywords: Access to maternity services; Ethnic minorities; Interpreter services; Maternal co-morbidities; Maternal death; Risk factors.
Crown Copyright © 2022 Published by Elsevier Ltd.
Conflict of interest statement
SK and MK are members of the MBRRACE-UK Collaboration. MK reports grants from Heathcare Quality Improvement Partnership, National Institute for Health Research MRC and Wellbeing of Women; MK has an honorarium for Hooker Distinguished Visiting Professorship McMaster University. SK reports a funded post from the University of Birmingham; is an NIHR grant holder, and is a collaborator on HQIP funded projects; was on the Steering Committee for NIHR funded trial- Impacted fetal head; was Chair on PreSePT Steering Committee of Health Foundation study; is Deputy Chair of HEE/NIHR Integrated Clinical Academic (ICA) Programme Pre-doctoral Clinical Academic Fellowship Scheme Panel. RN declares that this work was started while she was undertaking an intercalated degree in Public Health and Population Sciences at the University of Birmingham. MBRRACE provided study materials – access to case notes. EC declares that this work was started while she was undertaking an intercalated degree in Public Health and Population Sciences at the University of Birmingham. FCS declares that this work was completed while employed as a research fellow at the University of Birmingham - funded by the National Institute for Health Research (NIHR) Applied Research Collaborative (ARC) West Midlands – Maternity Theme.
Figures
Similar articles
-
A national cohort study and confidential enquiry to investigate ethnic disparities in maternal mortality.EClinicalMedicine. 2021 Dec 13;43:101237. doi: 10.1016/j.eclinm.2021.101237. eCollection 2022 Jan. EClinicalMedicine. 2021. PMID: 34977514 Free PMC article.
-
Project20: interpreter services for pregnant women with social risk factors in England: what works, for whom, in what circumstances, and how?Int J Equity Health. 2021 Oct 24;20(1):233. doi: 10.1186/s12939-021-01570-8. Int J Equity Health. 2021. PMID: 34689772 Free PMC article.
-
Pregnancy as an ideal time for intervention to address the complex needs of black and minority ethnic women: views of British midwives.Midwifery. 2015 Mar;31(3):373-9. doi: 10.1016/j.midw.2014.11.006. Epub 2014 Nov 13. Midwifery. 2015. PMID: 25483209
-
Role of ethnicity in high-level obstetric clinical incidents: a review of cases from a large UK NHS maternity unit.BMJ Open Qual. 2022 Nov;11(4):e001862. doi: 10.1136/bmjoq-2022-001862. BMJ Open Qual. 2022. PMID: 36379618 Free PMC article. Review.
-
Healthcare inequalities in antenatal care in the European Region: EBCOG Scientific review.Eur J Obstet Gynecol Reprod Biol. 2022 May;272:55-57. doi: 10.1016/j.ejogrb.2022.03.010. Epub 2022 Mar 3. Eur J Obstet Gynecol Reprod Biol. 2022. PMID: 35279642 Review.
Cited by
-
Provision of interpreting support for cross-cultural communication in UK maternity services: A Freedom of Information request.Int J Nurs Stud Adv. 2023 Nov 4;6:100162. doi: 10.1016/j.ijnsa.2023.100162. eCollection 2024 Jun. Int J Nurs Stud Adv. 2023. PMID: 38746811 Free PMC article.
-
Characteristics, outcomes, and maternity care experiences of women with children's social care involvement who subsequently died: national cohort study and confidential enquiry.BMJ Med. 2025 Jul 10;4(1):e001464. doi: 10.1136/bmjmed-2025-001464. eCollection 2025. BMJ Med. 2025. PMID: 40661818 Free PMC article.
References
-
- World Health Organization. The WHO application of ICD-10 to deaths during pregnancy, childbirth and puerperium: ICD MM. 2012. Available from: https://apps.who.int/iris/bitstream/handle/10665/70929/9789241548458_eng.... Accessed 14 January 2022.
-
- Kurinczuk JJ, Draper ES, Field DJ, et al. Experiences with maternal and perinatal death reviews in the UK—the MBRRACE-UK programme. 2014. Available from: https://onlinelibrary.wiley.com/doi/full/10.1111/1471-0528.12820. Accessed 14 January 2022. - DOI - PubMed
-
- National Quality Board. National guidance on learning from deaths. 2017. Available from: https://www.england.nhs.uk/wp-content/uploads/2017/03/nqb-national-guida.... Accessed 28 July 2021.
-
- World Health Organization. Maternal mortality. 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality. Accessed 14 January 2022.
LinkOut - more resources
Full Text Sources
