

Prenatal Diagnosis of Otocephaly: A Rare Facial Anomaly
- PMID: 35923505
- PMCID: PMC9339432
- DOI: 10.1007/s13224-021-01494-x
Prenatal Diagnosis of Otocephaly: A Rare Facial Anomaly
Abstract
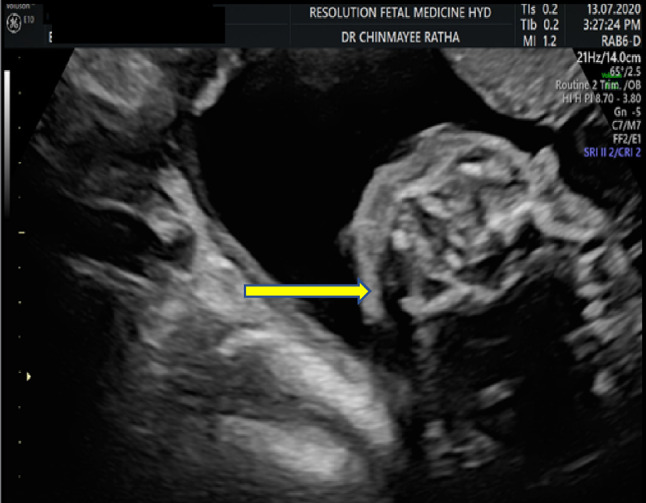
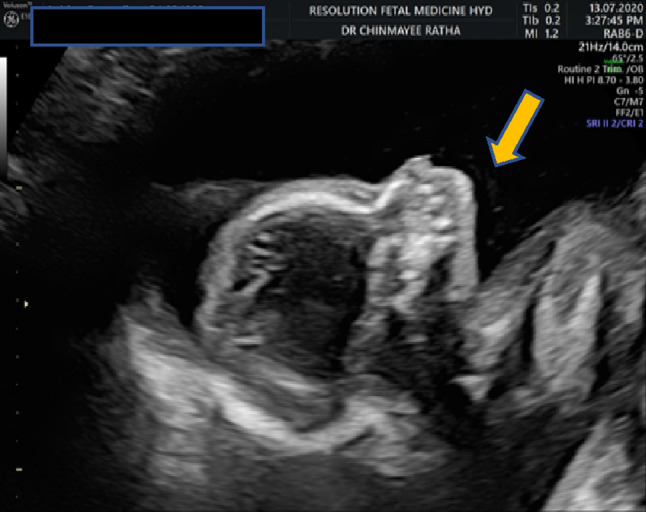
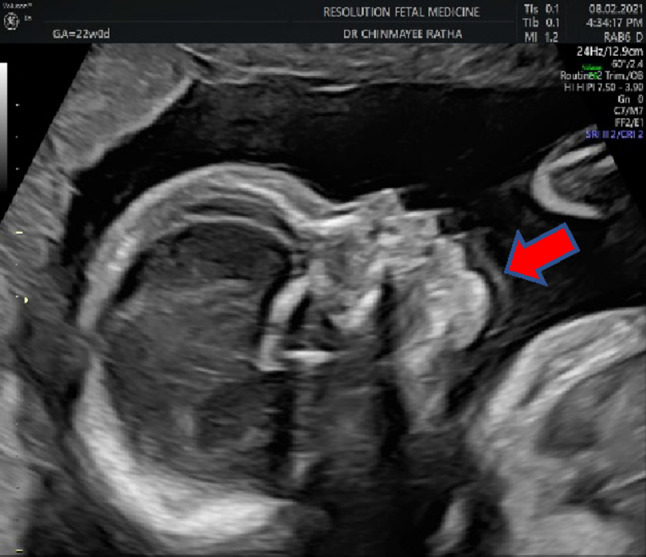
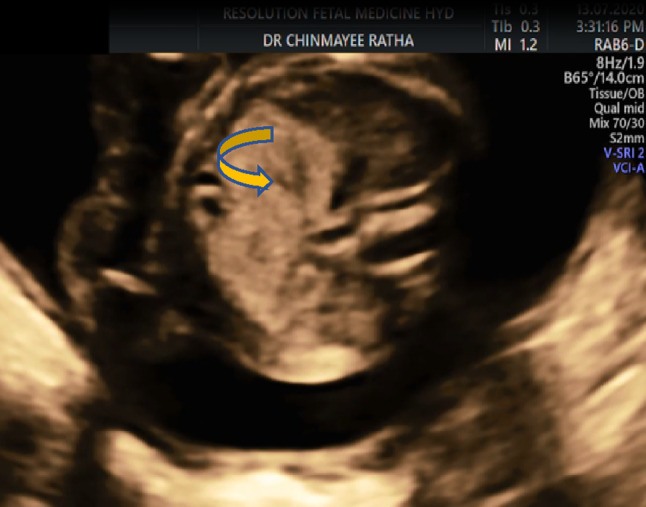
Introduction: Otocephaly is a rare malformation characterized by agnathia (absence of the mandible), melotia (medially displaced ear pinna), aglossia (absence of the tongue) and microstomia (small oral aperture). This results due to failure of migration of the neural crest cells and is a defect of the first branchial arch. It is incompatible with life and early prenatal diagnosis is useful.
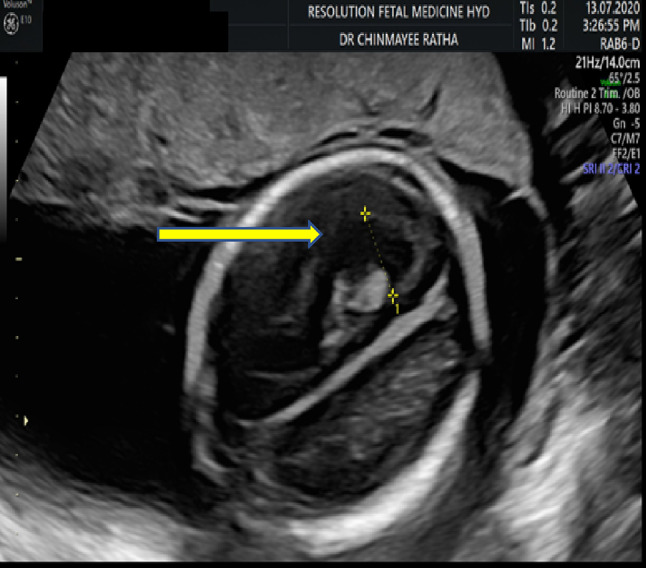
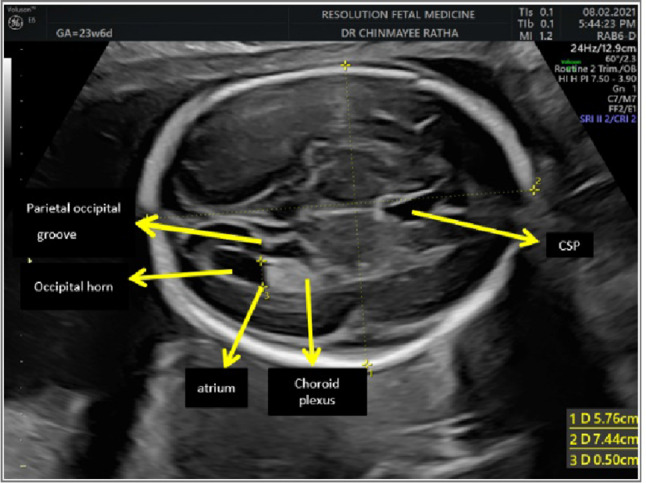
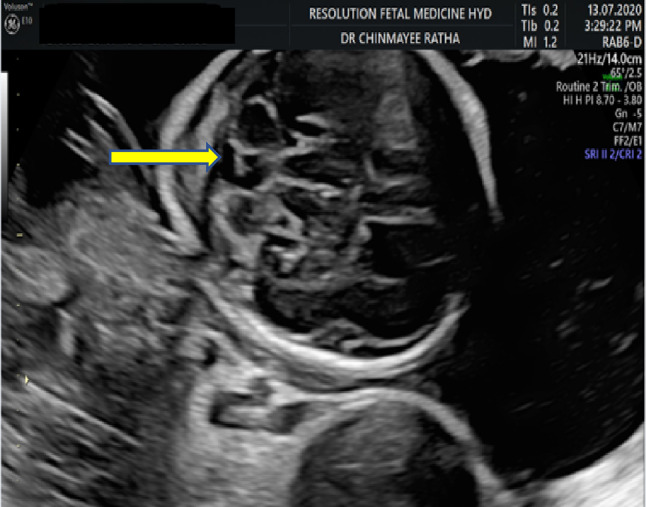
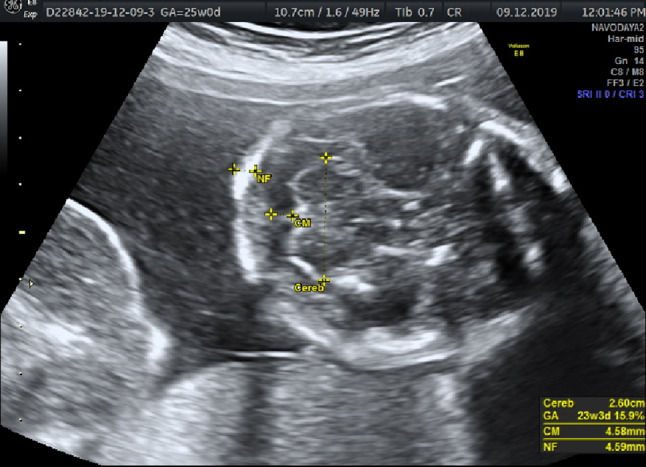
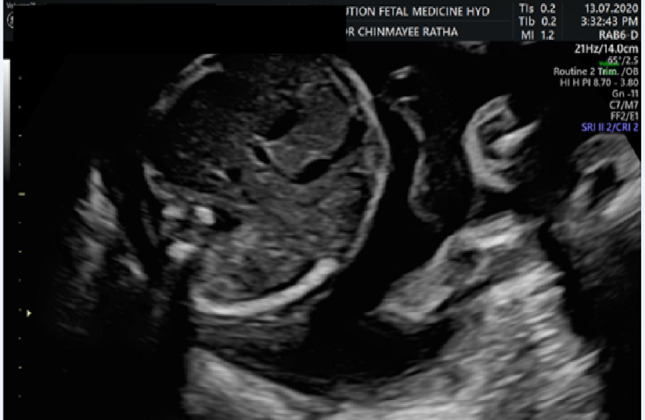
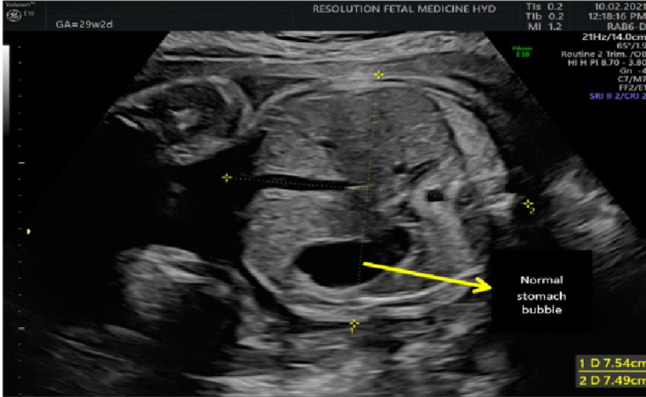
Case report: Our patient a primigravida with 19 weeks 6 days gestation was referred for micrognathia and polyhydramnios. On ultrasound examination, she had unilateral mild ventriculomegaly and posterior fossa cyst in the fetal brain. The fetus had agnathia and anophthalmia. There was an echogenic intracardiac focus and echogenic bowel. The stomach was not seen clearly. This could be due to agnathia and microstomia leading to swallowing difficulties. The patient was explained about the guarded prognosis. The pregnancy was terminated. A diagnosis of otocephaly was made.
Discussion: Otocephaly is a rare disorder of development of the first branchial arch. The reported incidence is 1 in 70,000. It is mostly lethal due to respiratory difficulties and may be associated with cranial and extracranial malformations. Most case reports have found that it is sporadic and could be due to mutations in the PRRX1 gene. Other anomalies that may be associated with otocephaly are neural tube defects, cephalocele, dysgenesis of corpus callosum, atresia of the third ventricle, midline probocis, hypotelorism, renal ectopia, cyclopia, vertebral and rib abnormalities, tracheo esophageal fistula, cardiac anomalies and adrenal hypoplasia. Most of the cases reported so far were diagnosed in the second or the third trimester. Facial anomaly screening has undergone a huge evolution in the recent years. In addition to the usual facial screening, we recommend mandibular arch screening in the first and early second trimester. If there is a doubt the patient may be called back at 15 to 16 weeks of gestation considering the fact that these anomalies are usually lethal and medical termination is safer earlier in pregnancy than later. MRI may be a handy tool to confirm antenatal diagnosis as it can detect the abnormal ears. Agnathia and polyhydramnios occur together in the third trimester but in the first or second trimester polyhydramnios may not be observed.
Conclusion: Otocephaly, though rare, poses a clinical challenge for both patient and the reporting doctor. Considering the time limitation for termination of pregnancy in our country, early prenatal diagnosis is important. A detailed face evaluation in the first trimester can help detect this defect as early as 11-14 weeks. Early diagnosis of lethal anomalies helps in completing the fetal work up and offering a safer termination. Correct diagnosis and work up of fetal anomalies allows for documentation and awareness of the presence of these conditions in our population.
Keywords: Agnathia; Anophthalmia; Melotia; Microstomia; Otocephaly; Synotia.
© Federation of Obstetric & Gynecological Societies of India 2021.
Conflict of interest statement
Conflict of interestThe authors have no conflicts of interest or any vested interests to declare.
Figures




Similar articles
-
Re-focusing on Agnathia-Otocephaly complex.Clin Oral Investig. 2021 Mar;25(3):1353-1362. doi: 10.1007/s00784-020-03443-w. Epub 2020 Jul 9. Clin Oral Investig. 2021. PMID: 32643087 Review.
-
Otocephaly: Agnathia- Microstomia-Synotia Syndrome- A Rare Congenital Anomaly.J Clin Diagn Res. 2015 Sep;9(9):ED03-4. doi: 10.7860/JCDR/2015/13636.6444. Epub 2015 Sep 1. J Clin Diagn Res. 2015. PMID: 26500912 Free PMC article.
-
Cyclopia: isolated and with agnathia-otocephaly complex.BMJ Case Rep. 2017 Aug 30;2017:bcr2017220159. doi: 10.1136/bcr-2017-220159. BMJ Case Rep. 2017. PMID: 28855214 Free PMC article.
-
Otocephaly: report of five new cases and a literature review.Fetal Pediatr Pathol. 2006 Sep-Oct;25(5):277-96. doi: 10.1080/15513810601123417. Fetal Pediatr Pathol. 2006. PMID: 17438667
-
Current perspectives on the etiology of agnathia-otocephaly.Eur J Med Genet. 2010 Nov-Dec;53(6):358-66. doi: 10.1016/j.ejmg.2010.09.002. Epub 2010 Sep 16. Eur J Med Genet. 2010. PMID: 20849990 Review.
Cited by
-
Isolated Agnathia-Otocephaly Complex Diagnosed Prenatally for Ex-Utero Intrapartum Treatment: A Case Report.Am J Case Rep. 2023 May 11;24:e939016. doi: 10.12659/AJCR.939016. Am J Case Rep. 2023. PMID: 37165610 Free PMC article.
Publication types
LinkOut - more resources
Full Text Sources