

Different types of Kounis syndrome caused by different episodes of bee sting anaphylaxis: Misfortunes never come singly
- PMID: 35923521
- PMCID: PMC9214853
- DOI: 10.1016/j.jccase.2022.03.002
Different types of Kounis syndrome caused by different episodes of bee sting anaphylaxis: Misfortunes never come singly
Abstract
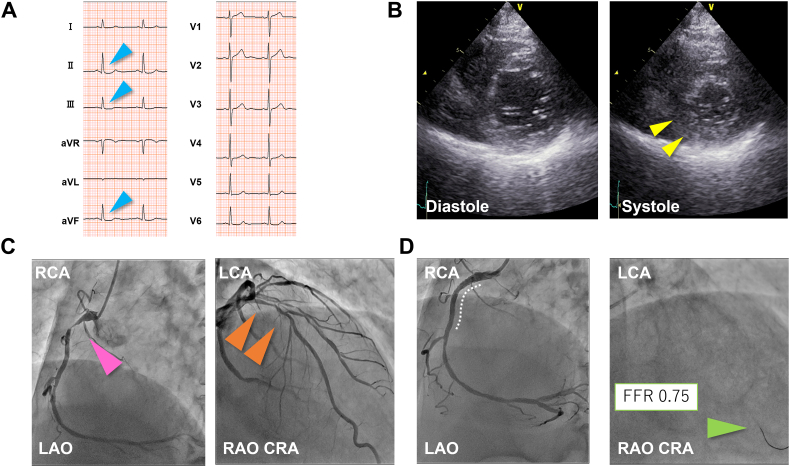
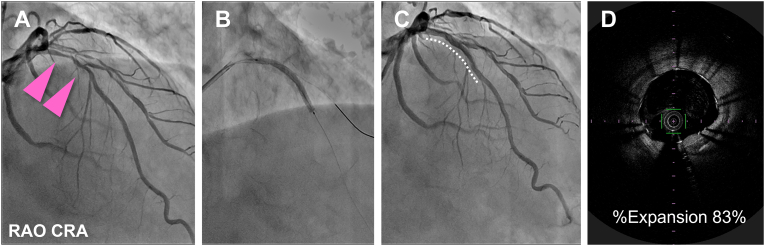
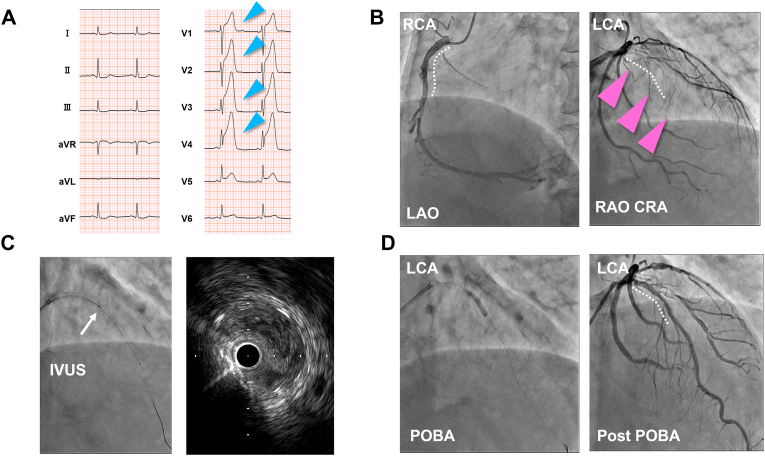
We report our experience with a 69-year-old man who had different types of Kounis syndrome over a short time frame, caused by two episodes of bee sting anaphylaxis. After his first allergic reaction to a bee sting, he experienced a non-ST-segment elevation myocardial infarction; he was treated with percutaneous coronary intervention for near-occlusion of his right coronary artery. This episode was deemed type 2 Kounis syndrome. Four weeks later, we electively treated the nonculprit residual stenosis in his left anterior descending artery. Unfortunately, 2 weeks after this elective procedure, he experienced anaphylactic shock due to a second bee sting. Electrocardiography showed ST elevation in the anterior leads, and emergent coronary angiography showed thrombotic occlusion of the newly implanted stent in the left anterior descending artery. This second episode was deemed type 3 Kounis syndrome.
Learning objectives: This is a rare example of different types of Kounis syndrome resulting from repeated exposures to an allergic source, an example that deepens our understanding of Kounis syndrome. This patient's experience illustrates the need for careful evaluation of the indications for revascularization of nonculprit lesions in patients with a history of Kounis syndrome.
Keywords: Case report; Kounis syndrome; ST elevation myocardial infarction; Stent thrombosis.
© 2022 Japanese College of Cardiology. Published by Elsevier Ltd. All rights reserved. All rights reserved.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Coronary Stent-Induced Kounis Syndrome: A Case Report.Cureus. 2025 Apr 29;17(4):e83208. doi: 10.7759/cureus.83208. eCollection 2025 Apr. Cureus. 2025. PMID: 40443635 Free PMC article.
-
Insight into the Time Course of Type III Kounis Syndrome: A Case Report.J Emerg Med. 2020 Aug;59(2):e65-e68. doi: 10.1016/j.jemermed.2020.04.054. Epub 2020 Jun 11. J Emerg Med. 2020. PMID: 32536494
-
Case Report: Anaphylactic shock and ST-elevation myocardial infarction following a bee sting: two deadly diseases in a patient with Kounis syndrome.Front Cardiovasc Med. 2025 May 12;12:1530829. doi: 10.3389/fcvm.2025.1530829. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40421190 Free PMC article.
-
Kounis syndrome caused by bee sting: a case report and literature review.Cardiovasc J Afr. 2023 Sep-Oct 23;34(4):256-259. doi: 10.5830/CVJA-2022-042. Epub 2022 Aug 29. Cardiovasc J Afr. 2023. PMID: 36044199 Free PMC article. Review.
-
Acute coronary syndrome secondary to allergic coronary vasospasm (Kounis Syndrome): a case series, follow-up and literature review.BMC Cardiovasc Disord. 2018 Feb 27;18(1):42. doi: 10.1186/s12872-018-0781-9. BMC Cardiovasc Disord. 2018. PMID: 29486712 Free PMC article. Review.
Cited by
-
Clinical complications in envenoming by Apis honeybee stings: insights into mechanisms, diagnosis, and pharmacological interventions.Front Immunol. 2024 Sep 18;15:1437413. doi: 10.3389/fimmu.2024.1437413. eCollection 2024. Front Immunol. 2024. PMID: 39359723 Free PMC article. Review.
-
Diagnosis of human envenoming by terrestrial venomous animals: Routine, advances, and perspectives.Toxicon X. 2024 Oct 10;24:100211. doi: 10.1016/j.toxcx.2024.100211. eCollection 2024 Dec. Toxicon X. 2024. PMID: 39507426 Free PMC article.
References
-
- Kounis N.G., Mazarakis A., Tsigkas G., Giannopoulos S., Goudevenos J. Kounis syndrome: a new twist on an old disease. Future Cardiol. 2011;7:805–824. - PubMed
-
- Abdelghany M., Subedi R., Shah S., Kozman H. Kounis syndrome: a review article on epidemiology, diagnostic findings, management and complications of allergic acute coronary syndrome. Int J Cardiol. 2017;232:1–4. - PubMed
-
- Mehta S.R., Wood D.A., Storey R.F., Mehran R., Bainey K.R., Nguyen H., et al. Complete revascularization with multivessel PCI for myocardial infarction. N Engl J Med. 2019;381:1411–1421. - PubMed
-
- Puymirat E., Cayla G., Simon T., Steg P.G., Montalescot G., Durand-Zaleski I., et al. Multivessel PCI guided by FFR or angiography for myocardial infarction. N Engl J Med. 2021;385:297–308. - PubMed
-
- Holmes D.R., Kereiakes D.J., Garg S., Serruys P.W., Dehmer G.J., Ellis S.G., et al. Stent thrombosis. J Am Coll Cardiol. 2010;56:1357–1365. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
