

The Association of Modifiable Postresuscitation Management and Annual Case Volume With Survival After Extracorporeal Cardiopulmonary Resuscitation
- PMID: 35923595
- PMCID: PMC9324623
- DOI: 10.1097/CCE.0000000000000733
The Association of Modifiable Postresuscitation Management and Annual Case Volume With Survival After Extracorporeal Cardiopulmonary Resuscitation
Abstract
It is not know if hospital-level extracorporeal cardiopulmonary resuscitation (ECPR) case volume, or postcannulation clinical management associate with survival outcomes.
Objectives: To describe variation in postresuscitation management practices, and annual hospital-level case volume, for patients who receive ECPR and to determine associations between these management practices and hospital survival.
Design: Observational cohort study using case-mix adjusted survival analysis.
Setting and participants: Adult patients greater than or equal to 18 years old who received ECPR from the Extracorporeal Life Support Organization Registry from 2008 to 2019.
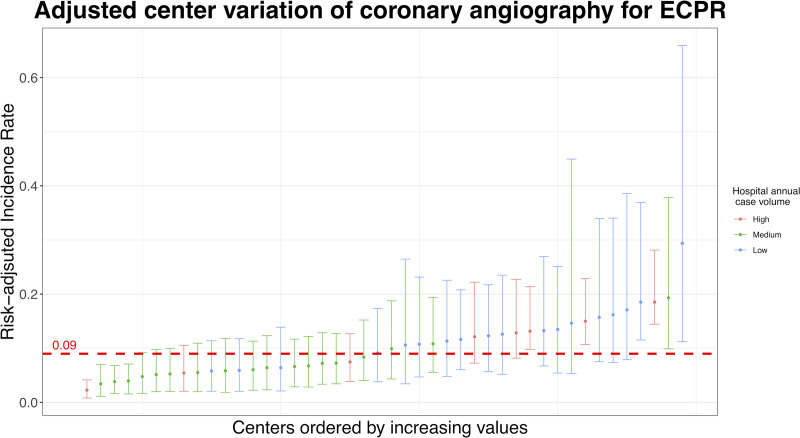
Main outcomes and measures: Generalized estimating equation logistic regression was used to determine factors associated with hospital survival, accounting for clustering by center. Factors analyzed included specific clinical management interventions after starting extracorporeal membrane oxygenation (ECMO) including coronary angiography, mechanical unloading of the left ventricle on ECMO (with additional placement of a peripheral ventricular assist device, intra-aortic balloon pump, or surgical vent), placement of an arterial perfusion catheter distal to the arterial return cannula (to mitigate leg ischemia); potentially modifiable on-ECMO hemodynamics (arterial pulsatility, mean arterial pressure, ECMO flow); plus hospital-level annual case volume for adult ECPR.
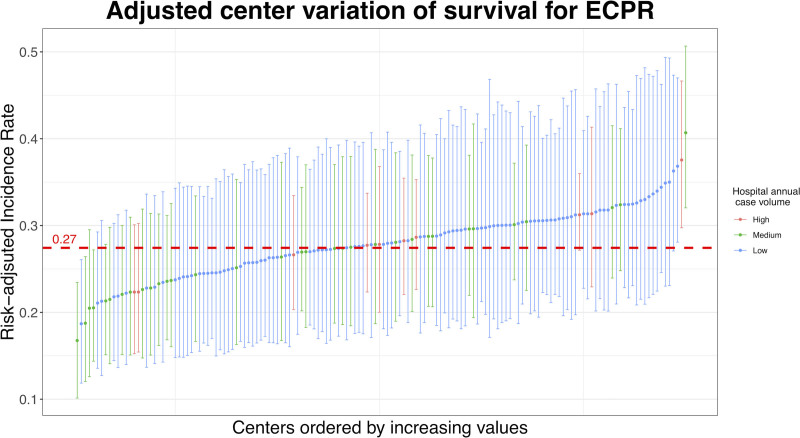
Results: Case-mix adjusted patient-level management practices varied widely across individual hospitals. We analyzed 7,488 adults (29% survival); median age 55 (interquartile range, 44-64), 68% of whom were male. Adjusted hospital survival on ECMO was associated with mechanical unloading of the left ventricle (odds ratio [OR], 1.3; 95% CI, 1.08-1.55; p = 0.005), performance of coronary angiography (OR, 1.34; 95% CI, 1.11- 1.61; p = 0.002), and placement of an arterial perfusion catheter distal to the return cannula (OR, 1.39; 95% CI, 1.05-1.84; p = 0.022). Survival varied by 44% across hospitals after case-mix adjustment and was higher at centers that perform more than 12 ECPR cases/yr (OR, 1.23; 95% CI, 1.04-1.45; p = 0.015) versus medium- and low-volume centers.
Conclusions and relevance: Modifiable ECMO management strategies and annual case volume vary across hospitals, appear to be associated with survival and should be the focus of future research to test if these hypothesis-generating associations are causal in nature.
Keywords: cardiac arrest; coronary angiography; critical care; extracorporeal cardiopulmonary resuscitation.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Figures
References
-
- Richardson AS, Schmidt M, Bailey M, et al. : ECMO cardio-pulmonary resuscitation (ECPR), trends in survival from an international multicentre cohort study over 12-years. Resuscitation 2017; 112:34–40 - PubMed
-
- Girotra S, Nallamothu BK, Tang Y, et al. ; American Heart Association Get With The Guidelines–Resuscitation Investigators: Association of hospital-level acute resuscitation and postresuscitation survival with overall risk-standardized survival to discharge for in-hospital cardiac arrest. JAMA Netw Open 2020; 3:e2010403. - PMC - PubMed
-
- Bernard SA, Gray TW, Buist MD, et al. : Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med 2002; 346:557–563 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
