

Opioid Prescribing Patterns Before, During, and After Critical Illness: An Observational Study
- PMID: 35923596
- PMCID: PMC9329077
- DOI: 10.1097/CCE.0000000000000735
Opioid Prescribing Patterns Before, During, and After Critical Illness: An Observational Study
Abstract
Objectives: The association between opioid therapy during critical illness and persistent opioid use after discharge is understudied relative to ICU opioid exposure and modifiable risk factors. Our objectives were to compare persistent opioid use after discharge among patients with and without chronic opioid use prior to admission (OPTA) and identify risk factors associated with persistent use.
Design: Retrospective cohort study.
Setting: Medical, trauma/surgical, or neurologic ICU at an academic hospital.
Participants: Adult patients surviving hospital admission.
Interventions: Opioid use during the ICU and post-ICU stays.
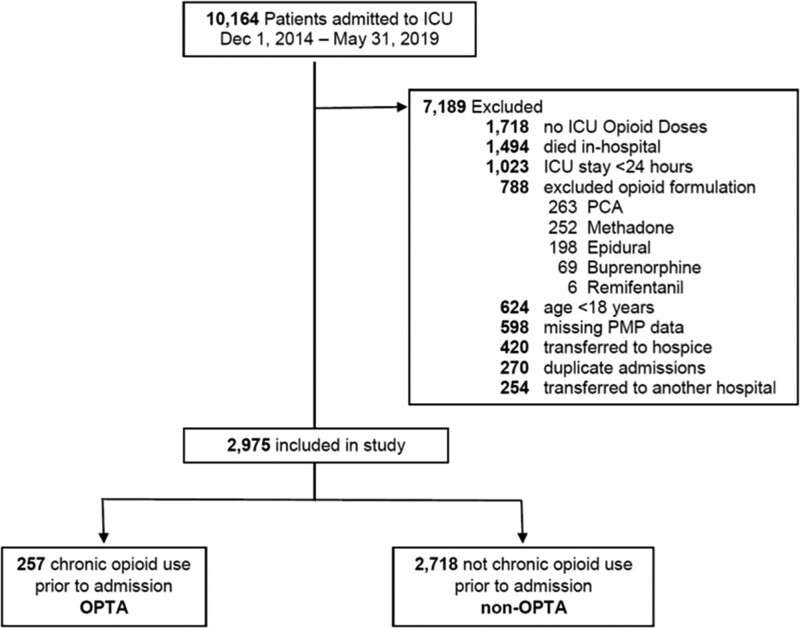
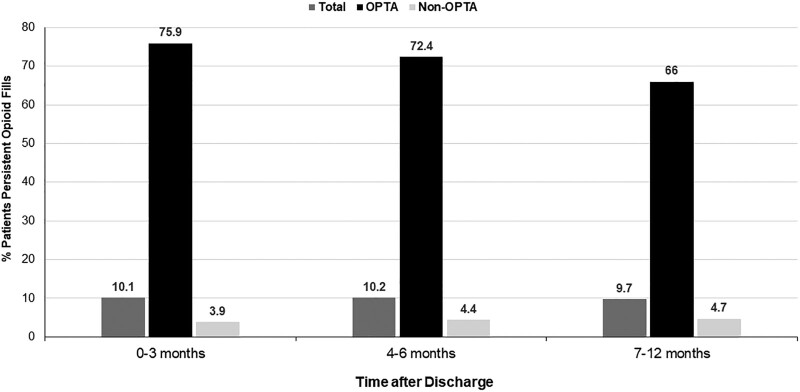
Measurements and main results: The primary outcome was persistent opioid use accounting for greater than 70% of days 4-6 months after discharge. Among 2,975 included patients, 257 (8.6%) were classified as OPTA, and 305 (10.2%) persistently filled opioid prescriptions, including 186/257 (72%) OPTA and 119/2,718 (4.4%) with no chronic opioid fills prior to admission. Among all patients, OPTA was strongly associated with persistent opioid use (odds ratio, 57.2 [95% CI, 41.4-80.0]). Multivariable logistic regression revealed that male sex, surgical procedure, and ICU opioid-free days were associated with reduced persistent opioid use for OPTA patients. Age and ICU opioid-free days were associated with reduced persistent opioid use for non-OPTA patients. Total ICU opioid dose and dose per day of ICU exposure were not associated with persistent use for either group.
Conclusions: In this mixed cohort of ICU patients, 10.2% persistently filled opioid prescriptions 4-6 months after discharge. Although ICU opioid doses were not associated with persistent use, duration of ICU opioid administration is a modifiable risk factor that may reduce persistent opioid use after critical illness.
Keywords: analgesia; analgesics; epidemic; intensive care unit; opioid; pain; sedation.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Figures
References
-
- Puntillo KA: Pain experiences of intensive care unit patients. Heart Lung 1990; 19:526–533 - PubMed
-
- Shapiro BA, Warren J, Egol AB, et al. : Practice parameters for intravenous analgesia and sedation for adult patients in the intensive care unit: An executive summary. Society of Critical Care Medicine. Crit Care Med 1995; 23:1596–1600 - PubMed
-
- Baker DW: History of The Joint Commission’s Pain Standards: Lessons for today’s prescription opioid epidemic. JAMA 2017; 317:1117–1118 - PubMed
-
- Jacobi J, Fraser GL, Coursin DB, et al. ; Task Force of the American College of Critical Care Medicine (ACCM) of the Society of Critical Care Medicine (SCCM), American Society of Health-System Pharmacists (ASHP), American College of Chest Physicians: Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med 2002; 30:119–141 - PubMed
-
- Porter J, Jick H: Addiction rare in patients treated with narcotics. N Engl J Med 1980; 302:123 - PubMed
LinkOut - more resources
Full Text Sources
