

Utility of Measuring Fetal Cavum Septum Pellucidum (CSP) Width During Routine Obstetrical Ultrasound for Improving Diagnosis of 22q11.2 Deletion Syndrome: A Case-Control Study
- PMID: 35923603
- PMCID: PMC9341354
- DOI: 10.2147/TACG.S364543
Utility of Measuring Fetal Cavum Septum Pellucidum (CSP) Width During Routine Obstetrical Ultrasound for Improving Diagnosis of 22q11.2 Deletion Syndrome: A Case-Control Study
Abstract
Objective: To evaluate the utility of measuring fetal cavum septum pellucidum (CSP) width during routine, mid-pregnancy ultrasound for improving diagnosis of 22q11.2 deletion syndrome amongst fetuses with and without conotruncal anomalies.
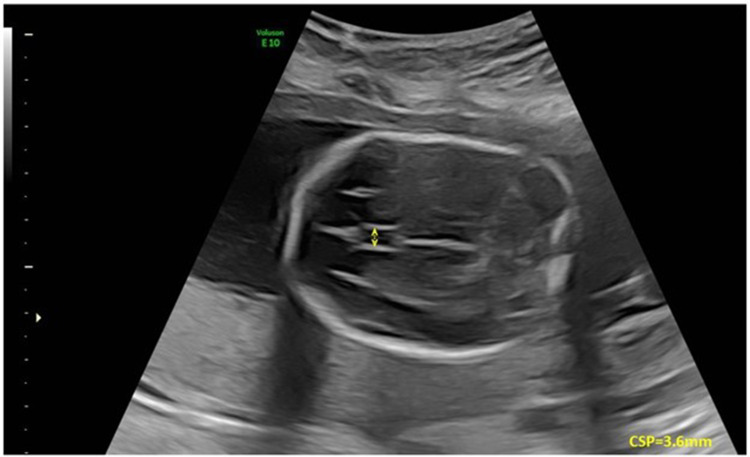
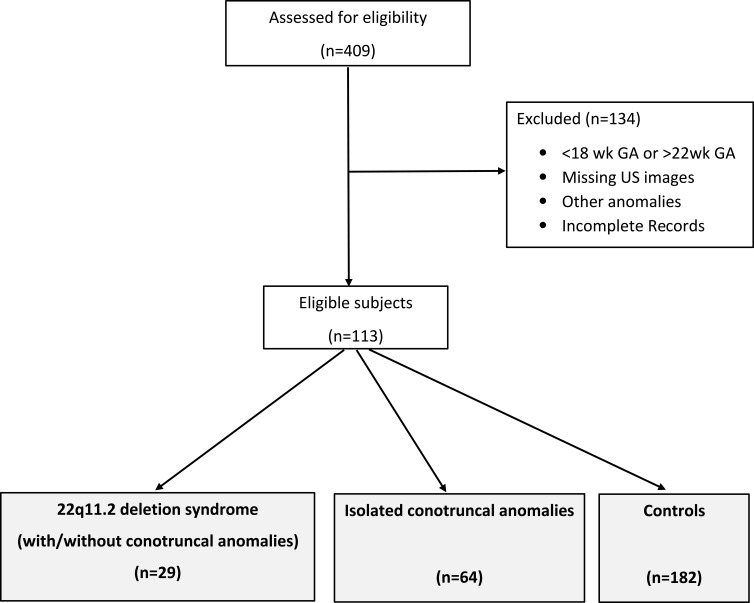
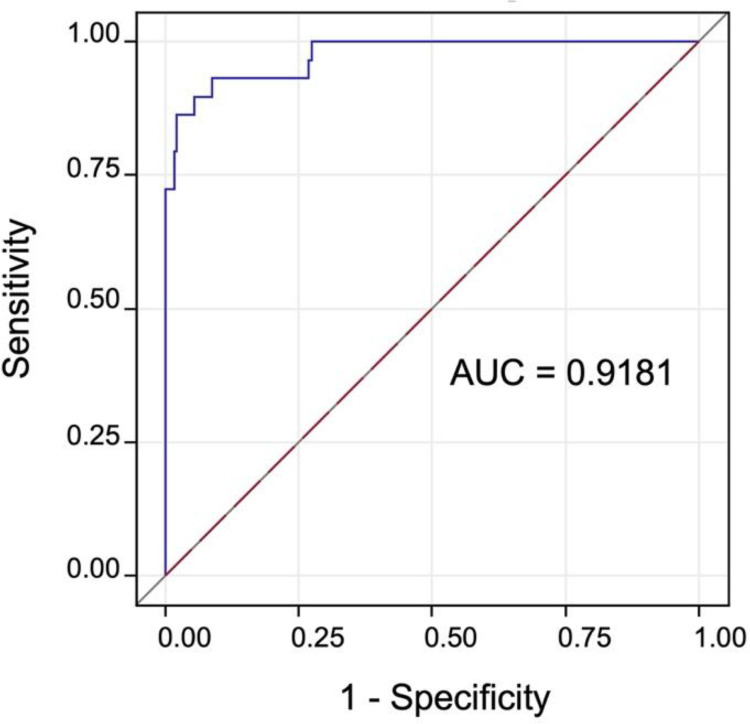
Patients and methods: This was a retrospective case-control study (2005-2016). Fetuses and newborns with 22q11.2 deletion and/or conotruncal cardiac anomalies were identified using a regional, clinical database. A control group was assembled in a 2:1 ratio to create three groups for comparison: i) 22q11.2 deletion syndrome; ii) isolated conotruncal anomalies; and iii) controls. Eligibility was restricted to those with stored ultrasound images between 18-22 weeks' gestation and a minimum biparietal diameter of 40 mm. Post-processing measurement of CSP width was performed in a standardized fashion by two blinded and independent study personnel. Descriptive and inferential statistics, regression modeling, and receiver operator curves (ROC) were used to compare outcomes between groups and evaluate sensitivity/specificity of CSP width as a marker of 22q11.2 deletion syndrome.
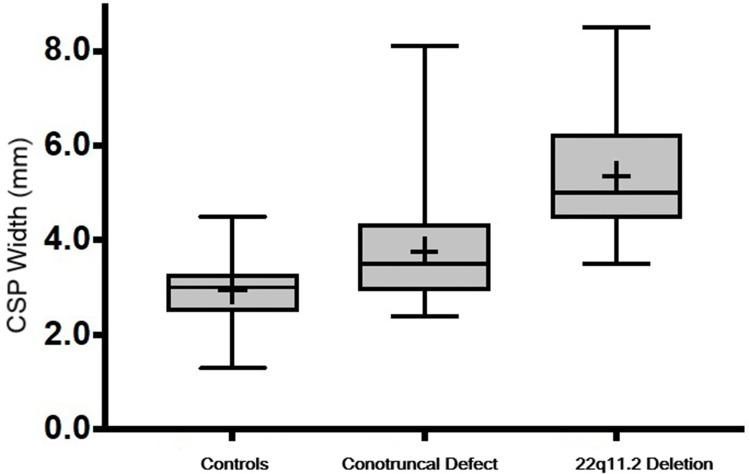
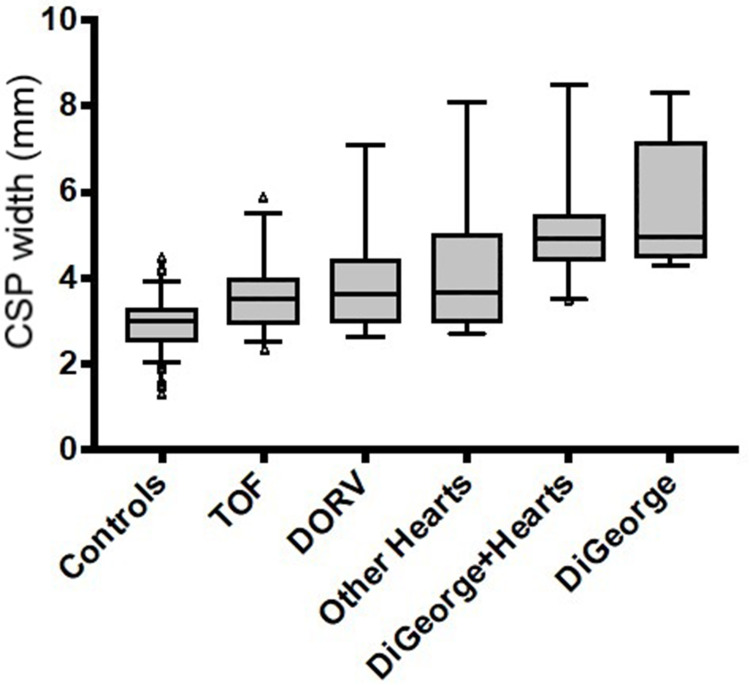
Results: Twenty-nine cases of 22q11.2 deletion and 64 cases of isolated conotruncal anomalies were matched to 186 healthy controls. Cases with 22q11.2 deletion syndrome had significantly larger CSP widths (5.36 mm; SD=1.2) compared to those with isolated conotruncal anomalies (3.75 mm; SD=1.11) and healthy controls (2.93 mm; SD=0.57; p<0.0001). There was no difference in CSP width amongst those with 22q11.2 deletion irrespective of the presence/absence of a conotruncal anomaly (p=0.362), or by type of conotruncal anomaly (p=0.211). Using a CSP width cutoff >4.3 mm, fetuses with 22q11.2 deletion can be accurately identified with good sensitivity (89.7%) and specificity (84%).
Conclusion: Fetuses with 22q11.2 deletion syndrome have dilated CSPs when compared to those with isolated conotruncal anomalies or controls. Because CSP dilation can be evaluated during routine mid-pregnancy ultrasound using standard images of the fetal head, measurement could easily be incorporated to enhance prenatal diagnosis of this phenotypically diverse condition.
Keywords: 22q11 microdeletion; DiGeorge syndrome; cavum septum pellucidum; fetal ultrasound; neurosonography; prenatal diagnosis.
© 2022 Pylypjuk et al.
Conflict of interest statement
The authors report no conflicts of interest in this work. Dr. Christy Pylypjuk has received grants from the Manitoba Medical Services Foundation and Children’s Hospital Research Institute of Manitoba, Health Sciences Centre Foundation, University of Manitoba, and the Winnipeg Foundation Martha Donovan Women’s Leadership Award, as well as transportation and lodging to speak at the annual conference of the Society of Obstetricians and Gynecologists of Canada (no direct payments were received), outside of the submitted work.
Figures
Similar articles
-
Prenatal Screening and Diagnostic Considerations for 22q11.2 Microdeletions.Genes (Basel). 2023 Jan 6;14(1):160. doi: 10.3390/genes14010160. Genes (Basel). 2023. PMID: 36672900 Free PMC article. Review.
-
Enlarged cavum septum pellucidum and small thymus as markers for 22q11.2 deletion syndrome.Prenat Diagn. 2024 Jun;44(6-7):796-803. doi: 10.1002/pd.6555. Epub 2024 Mar 18. Prenat Diagn. 2024. PMID: 38497811
-
Dilated cavum septi pellucidi in fetuses with microdeletion 22q11.Prenat Diagn. 2016 Oct;36(10):911-915. doi: 10.1002/pd.4911. Epub 2016 Aug 30. Prenat Diagn. 2016. PMID: 27502038
-
Comparison of Cavum Septum Pellucidum Size in Euploid and Aneuploid Fetuses.Rev Bras Ginecol Obstet. 2023 Sep;45(9):e511-e516. doi: 10.1055/s-0043-1775847. Epub 2023 Oct 16. Rev Bras Ginecol Obstet. 2023. PMID: 37846183 Free PMC article.
-
Evaluation and Significance of Nonvisualization of the Cavum Septum Pellucidum on Prenatal Ultrasonography.Obstet Gynecol Surv. 2024 Aug;79(8):477-483. doi: 10.1097/OGX.0000000000001296S. Obstet Gynecol Surv. 2024. PMID: 39136638 Review.
Cited by
-
Prenatal cardiac findings and 22q11.2 deletion syndrome: Fetal detection and evaluation.Prenat Diagn. 2024 Jun;44(6-7):804-814. doi: 10.1002/pd.6566. Epub 2024 Apr 9. Prenat Diagn. 2024. PMID: 38593251 Free PMC article. Review.
-
Prenatal Screening and Diagnostic Considerations for 22q11.2 Microdeletions.Genes (Basel). 2023 Jan 6;14(1):160. doi: 10.3390/genes14010160. Genes (Basel). 2023. PMID: 36672900 Free PMC article. Review.
-
FetSAM: Advanced Segmentation Techniques for Fetal Head Biometrics in Ultrasound Imagery.IEEE Open J Eng Med Biol. 2024 Mar 27;5:281-295. doi: 10.1109/OJEMB.2024.3382487. eCollection 2024. IEEE Open J Eng Med Biol. 2024. PMID: 38766538 Free PMC article.
-
Clinical Course and Outcome of Prenatally Detected 22q11.2 Deletion Syndrome-A Retrospective Analysis.Diagnostics (Basel). 2023 Jul 1;13(13):2244. doi: 10.3390/diagnostics13132244. Diagnostics (Basel). 2023. PMID: 37443638 Free PMC article.
References
LinkOut - more resources
Full Text Sources
