

A glance into the future of gout
- PMID: 35923650
- PMCID: PMC9340313
- DOI: 10.1177/1759720X221114098
A glance into the future of gout
Abstract
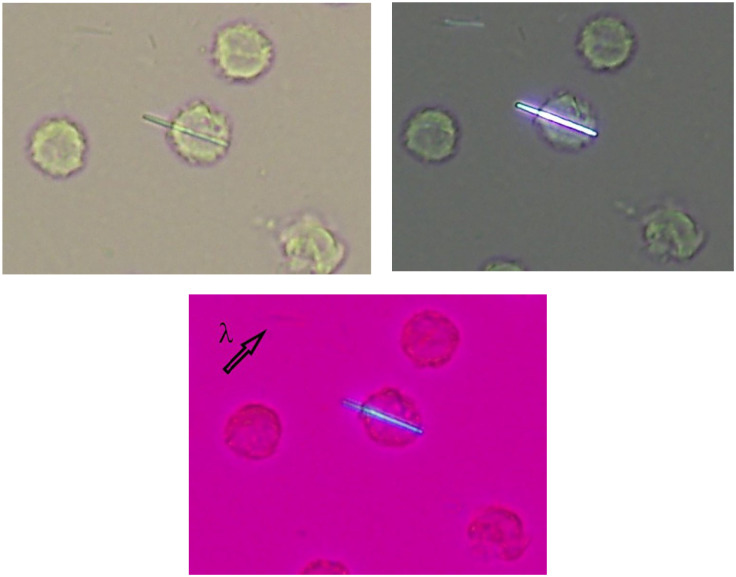
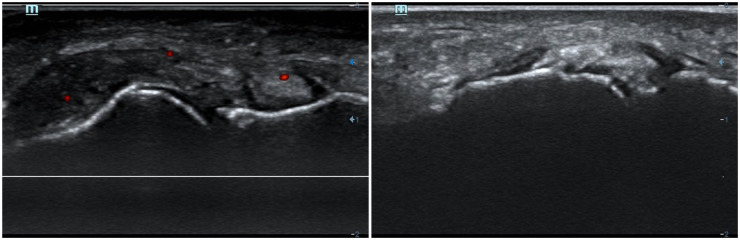
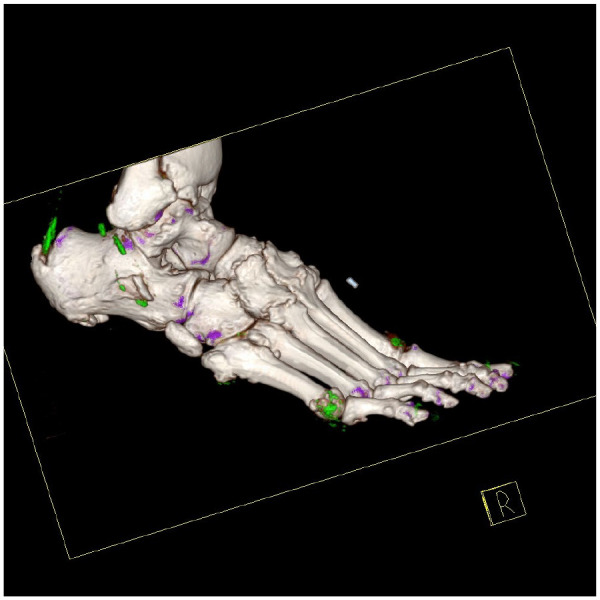
Gout is characterized by monosodium urate (MSU) crystal deposits in and within joints. These deposits result from persistent hyperuricaemia and most typically lead to recurrent acute inflammatory episodes (gout flares). Even though some aspects of gout are well characterized, uncertainties remain; this upcoming decade should provide further insights into many of these uncertainties. Synovial fluid analysis allows for the identification of MSU crystals and unequivocal diagnosis. Non-invasive methods for diagnosis are being explored, such as Raman spectroscopy and imaging modalities. Both ultrasound and dual-energy computed tomography (DECT) allow the detection of MSU crystals; this not only provides a mean of diagnosis, but also has furthered gout knowledge defining the presence of a preclinical deposition in asymptomatic hyperuricaemia. Scientific consensus establishes the beginning of gout as the beginning of symptoms (usually the first flare), but the concept is currently under review. For effective long-term gout management, the main goal is to promote crystal dissolution treatment by reducing serum urate below 6 mg/dL (or 5 mg/dL if faster crystal dissolution is required). Current urate-lowering therapies' (ULTs) options are limited, with allopurinol and febuxostat being widely available, and probenecid, benzbromarone, and pegloticase available in some regions. New xanthine oxidase inhibitors and, especially, uricosurics inhibiting urate transporter URAT1 are under development; it is probable that the new decade will see a welcomed increase in the gout therapeutic armamentarium. Cardiovascular and renal comorbidities are common in gout patients. Studies determining whether optimal treatment of gout will positively impact these comorbidities are currently lacking, but will hopefully be forthcoming. Overall, the single change that will most impact gout management is greater uptake of international rheumatology society recommendations. Innovative strategies, such as nurse-led interventions based on these recommendations have recently demonstrated treatment success for people with gout.
Keywords: diagnosis; gout; pathogenesis; treatment; urate.
© The Author(s), 2022.
Conflict of interest statement
Competing Interests: The authors declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: FS reports research grants from Novartis and speaking fees from Menarini. M. A. reports research grants from Grünenthal and speaking fees from Menarini. N.D. reports grants from AstraZeneca and Amgen, consulting fees from Dyve BioSciences, AstraZeneca JW Pharmaceuticals, Selecta, Arthrosi, Horizon, and PK Med, and speaker fees from Abbvie and Janssen.
Figures
References
-
- Dehlin M, Jacobsson L, Roddy E. Global epidemiology of gout: prevalence, incidence, treatment patterns and risk factors. Nat Rev Rheumatol 2020; 16: 380–390. - PubMed
-
- Dalbeth N, Pool B, Gamble GD, et al. Cellular characterization of the gouty tophus: a quantitative analysis. Arthritis Rheum 2010; 62: 1549–1556. - PubMed
-
- Macfarlane DG, Dieppe PA. Diuretic induced gout in elderly women. Br J Rheumatol 1985; 24: 155–157. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
