

A Comparation Between Frame-Based and Robot-Assisted in Stereotactic Biopsy
- PMID: 35923834
- PMCID: PMC9339900
- DOI: 10.3389/fneur.2022.928070
A Comparation Between Frame-Based and Robot-Assisted in Stereotactic Biopsy
Abstract
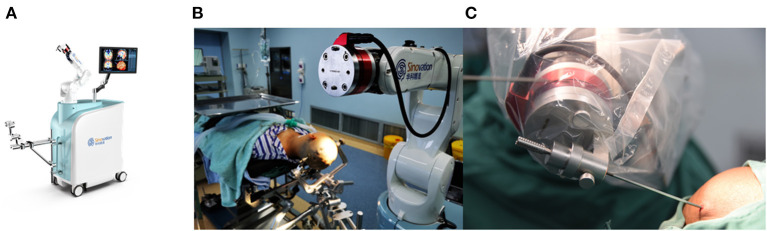
Introduction: Frame-based stereotactic biopsy is well-established to play an essential role in neurosurgery. In recent years, different robotic devices have been introduced in neurosurgery centers. This study aimed to compare the SINO surgical robot-assisted frameless brain biopsy with standard frame-based stereotactic biopsy in terms of efficacy, accuracy and complications.
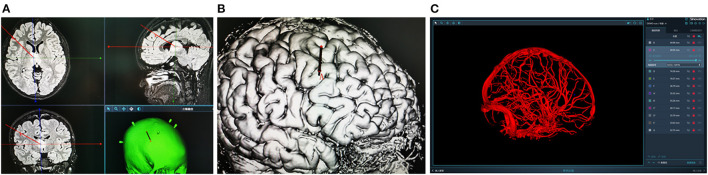
Methods: A retrospective analysis was performed on 151 consecutive patients who underwent stereotactic biopsy at Chongqing Sanbo Jiangling Hospital between August 2017 and December 2021. All patients were divided into the frame-based group (n = 47) and the SINO surgical robot-assisted group (n = 104). The data collected included clinical characteristics, diagnostic yield, operation times, accuracy, and postoperative complications.
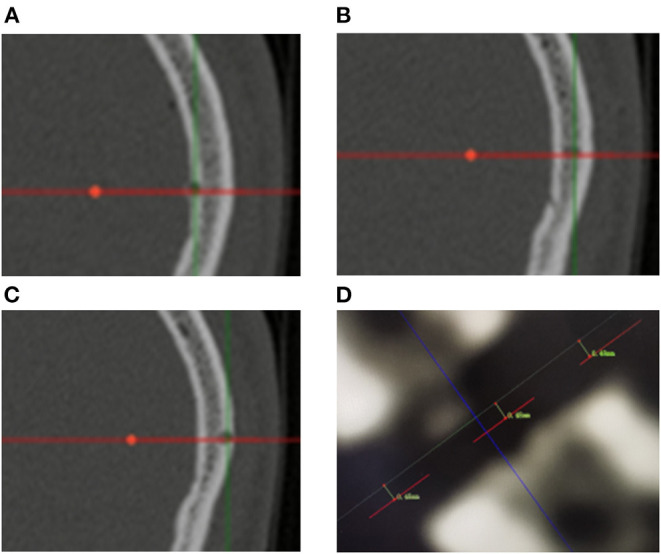
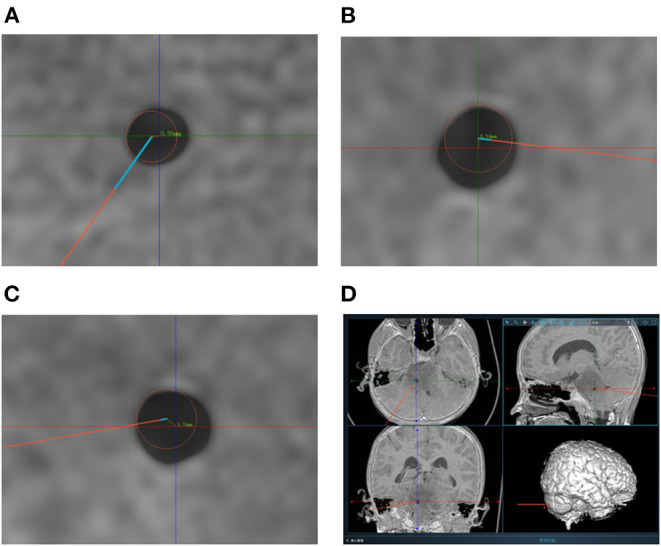
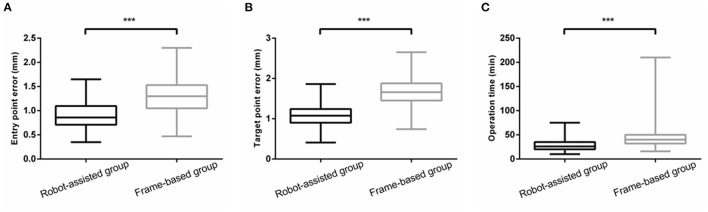
Results: There was no significant difference in diagnostic yield between the frame-based group and the SINO surgical robot-assisted group (95.74 vs. 98.08%, p > 0.05). The mean operation time in the SINO surgical robot-assisted group was significantly shorter than in the frame-based group (29.36 ± 13.64 vs. 50.57 ± 41.08 min). The entry point error in the frame-based group was significantly higher than in the robot-assisted group [1.33 ± 0.40 mm (0.47-2.30) vs. 0.92 ± 0.27 mm (0.35-1.65), P < 0.001]. The target point error in the frame-based group was also significantly higher than in the robot-assisted group [1.63 ± 0.41 mm (0.74-2.65) vs. 1.10 ± 0.30 mm (0.69-2.03), P < 0.001]. Finally, there was no significant difference in postoperative complications between the two groups.
Conclusion: Robot-assisted brain biopsy becomes an increasingly mainstream tool in the neurosurgical procedure. The SINO surgical robot-assisted platform is as efficient, accurate and safe as standard frame-based stereotactic biopsy and provides a reasonable alternative to stereotactic biopsy in neurosurgery.
Keywords: SINO robot; brain biopsy; frameless stereotactic biopsy; intracranial lesions; robot-assisted surgery.
Copyright © 2022 Hu, Cai, Zhang, Adilijiang, Peng, Li, Che, Lan and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Robot-assisted stereotactic brain biopsy: A systematic review and meta-analysis.Neurosurg Rev. 2024 Dec 4;47(1):886. doi: 10.1007/s10143-024-03122-4. Neurosurg Rev. 2024. PMID: 39627622
-
A Comparison of the Safety, Efficacy, and Accuracy of Frame-Based versus Remebot Robot-Assisted Stereotactic Systems for Biopsy of Brainstem Tumors.Brain Sci. 2023 Feb 20;13(2):362. doi: 10.3390/brainsci13020362. Brain Sci. 2023. PMID: 36831906 Free PMC article.
-
Comparative Analysis of Efficacy and Safety of Frame-Based, Frameless, and Robot-Assisted Stereotactic Brain Biopsies: A Systematic Review and Meta-Analysis.Oper Neurosurg. 2025 Jun 1;28(6):749-761. doi: 10.1227/ons.0000000000001408. Epub 2024 Nov 7. Oper Neurosurg. 2025. PMID: 40062857
-
A comparison of the efficacy, safety, and duration of frame-based and Remebot robot-assisted frameless stereotactic biopsy.Br J Neurosurg. 2021 Jun;35(3):319-323. doi: 10.1080/02688697.2020.1812519. Epub 2020 Sep 17. Br J Neurosurg. 2021. PMID: 32940070
-
A Bulk Retrospective Study of Robot-Assisted Stereotactic Biopsies of Intracranial Lesions Guided by Videometric Tracker.Front Neurol. 2021 Aug 4;12:682733. doi: 10.3389/fneur.2021.682733. eCollection 2021. Front Neurol. 2021. PMID: 34421791 Free PMC article.
Cited by
-
Novel application of robot-guided stereotactic technique on biopsy diagnosis of intracranial lesions.Front Neurol. 2023 Jul 27;14:1173776. doi: 10.3389/fneur.2023.1173776. eCollection 2023. Front Neurol. 2023. PMID: 37576012 Free PMC article.
-
Neurosurgical robots in China: State of the art and future prospect.iScience. 2023 Sep 21;26(11):107983. doi: 10.1016/j.isci.2023.107983. eCollection 2023 Nov 17. iScience. 2023. PMID: 37867956 Free PMC article. Review.
-
Robot-assisted stereotactic brain biopsy: A systematic review and meta-analysis.Neurosurg Rev. 2024 Dec 4;47(1):886. doi: 10.1007/s10143-024-03122-4. Neurosurg Rev. 2024. PMID: 39627622
-
Robot-assisted versus manually guided stereotactic biopsy for intracranial lesions - a systematic review and meta-analysis.Neurosurg Rev. 2024 Nov 30;47(1):880. doi: 10.1007/s10143-024-03121-5. Neurosurg Rev. 2024. PMID: 39615014
-
Diagnostic yield of intraoperative frozen sections obtained through robot-assisted stereotactic biopsy of brain lesions.Front Neurol. 2025 Jun 10;16:1544613. doi: 10.3389/fneur.2025.1544613. eCollection 2025. Front Neurol. 2025. PMID: 40556650 Free PMC article.
References
LinkOut - more resources
Full Text Sources