

A Rare Case of Multicentric Primary Pulmonary Artery Sarcoma: Eliminating the Masquerade with Multimodality Imaging
- PMID: 35924130
- PMCID: PMC9340182
- DOI: 10.1055/s-0042-1744139
A Rare Case of Multicentric Primary Pulmonary Artery Sarcoma: Eliminating the Masquerade with Multimodality Imaging
Abstract
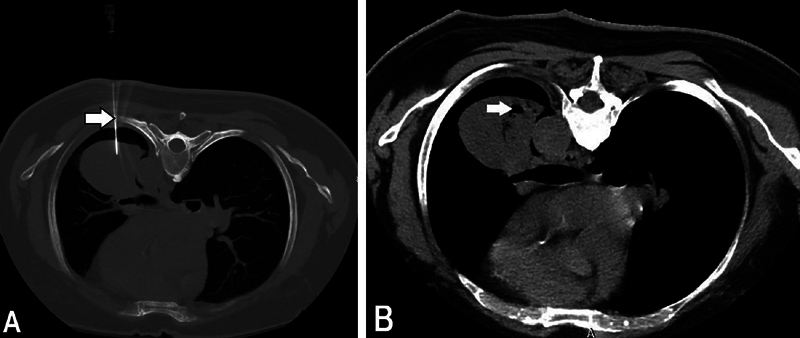
A 68-year-old male presented with a short history of exertional dyspnea and a provisional diagnosis of pulmonary thromboembolism was made. However, chest radiograph and further investigations in the form of computed tomography pulmonary angiogram, magnetic resonance imaging of thorax, and whole body fluorodeoxyglucose (FDG) positron emission tomography-computed tomography revealed a large mass arising from the distal left pulmonary artery extending into adjacent lung and another lesion near the root of the main pulmonary artery, both of which showed post-contrast enhancement and intense FDG uptake. Tissue sampling by transthoracic computed tomography-guided biopsy and immunohistochemistry confirmed the diagnosis of pulmonary artery angiosarcoma. Here, we present such a case of very rare occurrence which, in view of multicentricity and substantial extension into adjacent lung, is the first of its kind to be reported, to the best of our knowledge.
Keywords: PAS; angiosarcoma; pulmonary artery sarcoma; sarcoma; wall eclipsing sign.
Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest The authors declare that they have no conflict of interest.
Figures





Similar articles
-
A case report of pulmonary artery intimal sarcoma negative for 18F-FDG mimicking pulmonary thromboembolism.Eur Heart J Case Rep. 2023 Apr 26;7(4):ytad140. doi: 10.1093/ehjcr/ytad140. eCollection 2023 Apr. Eur Heart J Case Rep. 2023. PMID: 37123654 Free PMC article.
-
A primary pulmonary artery sarcoma masquerading pulmonary embolism: a case report and literature review.Thromb J. 2024 Jan 4;22(1):4. doi: 10.1186/s12959-023-00578-0. Thromb J. 2024. PMID: 38178144 Free PMC article.
-
Spindle cell sarcoma of pulmonary artery mimicking thromboembolism with lung metastasis detected in fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography.Indian J Nucl Med. 2014 Oct;29(4):249-51. doi: 10.4103/0972-3919.142631. Indian J Nucl Med. 2014. PMID: 25400365 Free PMC article.
-
Right atrial epithelioid angiosarcoma with multiple pulmonary metastasis confirmed by multimodality imaging-guided pulmonary biopsy: A case report and literature review.Medicine (Baltimore). 2018 Jul;97(30):e11588. doi: 10.1097/MD.0000000000011588. Medicine (Baltimore). 2018. PMID: 30045289 Free PMC article. Review.
-
Primary pulmonary artery sarcoma with intrapulmonary metastases based on PET/CT imaging: a case report and literature review.Ann Palliat Med. 2021 Jun;10(6):7013-7018. doi: 10.21037/apm-20-630. Epub 2020 Nov 18. Ann Palliat Med. 2021. PMID: 33222446 Review.
Cited by
-
Pulmonary Vein Stenosis after Catheter Ablation for Atrial Fibrillation: An Early Diagnosis Using Unenhanced Computed Tomography.Intern Med. 2024 May 15;63(10):1443-1449. doi: 10.2169/internalmedicine.2289-23. Epub 2023 Oct 6. Intern Med. 2024. PMID: 37813617 Free PMC article.
References
-
- Bleisch V R, Kraus F T. Polypoid sarcoma of the pulmonary trunk: analysis of the literature and report of a case with leptomeric organelles and ultrastructural features of rhabdomyosarcoma. Cancer. 1980;46(02):314–324. - PubMed
-
- Bendel E C, Maleszewski J J, Araoz P A. Imaging sarcomas of the great vessels and heart. Semin Ultrasound CT MR. 2011;32(05):377–404. - PubMed
-
- Nonomura A, Kurumaya H, Kono N et al.Primary pulmonary artery sarcoma. Report of two autopsy cases studied by immunohistochemistry and electron microscopy, and review of 110 cases reported in the literature. Acta Pathol Jpn. 1988;38(07):883–896. - PubMed
Publication types
LinkOut - more resources
Full Text Sources