

How Are Imaging Findings Associated with Exocrine Insufficiency in Idiopathic Chronic Pancreatitis?
- PMID: 35924133
- PMCID: PMC9340190
- DOI: 10.1055/s-0042-1744138
How Are Imaging Findings Associated with Exocrine Insufficiency in Idiopathic Chronic Pancreatitis?
Abstract
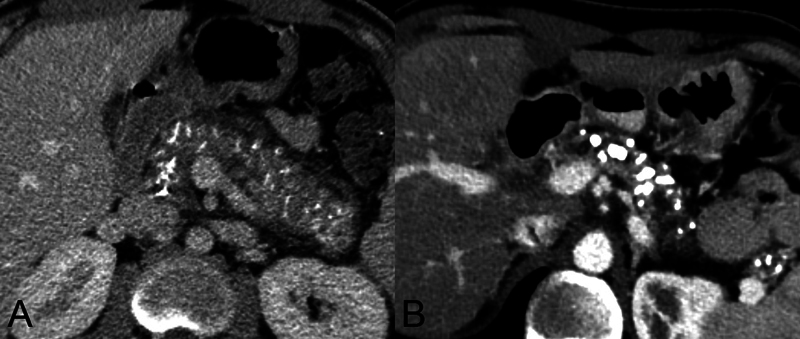
Aim The aim is to study the association between imaging findings in chronic pancreatitis and fecal elastase 1 (FE1) in patients with idiopathic chronic pancreatitis (ICP). Methods In this retrospective study on a prospectively maintained database of patients with ICP, a radiologist blinded to clinical and laboratory findings reviewed CT and/or MRI. Findings were documented according to recommendations of the Consortium for the Study of Chronic Pancreatitis, Diabetes, and Pancreatic Cancer, October 2018. Low FE1 (<100 μg elastase/g) was considered diagnostic of pancreatic exocrine insufficiency (PEI). Association between imaging findings and FE1 was studied. Results In total, 70 patients (M: F = 37:33) with ICP with mean age of 24.2 (SD 6.5) years, range 10 to 37 years and mean disease duration of 5.6 (SD 4.6) years, range 0 to 20 years were included. Mean FE level was 82.5 (SD 120.1), range 5 to 501 μg elastase/g. Mean main pancreatic duct (MPD) caliber was 7 (SD 4) mm, range 3 to 21 mm and mean pancreatic parenchymal thickness (PPT) was 13.7 (SD 5.5) mm, range 5 to 27 mm. There was a significant association between FE1 and MPD size, PPT, type of pancreatic calcification; presence of intraductal stones, side branch dilatation on magnetic resonance cholangiopancreatography and extent of pancreatic involvement ( p <0.05). In total, 79%, 86%, and 78% with moderate to severe MPD dilatation, pancreatic atrophy, and side branch dilatation had low FE1, respectively. But nearly half of those with no or mild structural abnormality on imaging had low FE1. Conclusion Significant association between FE1 and specific imaging findings demonstrates its potential as a marker of exocrine insufficiency and disease severity in chronic pancreatitis. But imaging and FE1 are complementary rather than supplementary.
Keywords: CT; MRI; chronic pancreatitis; fecal elastase 1; pancreatic exocrine insufficiency.
Indian Radiological Association. This is an open access article published by Thieme under the terms of the Creative Commons Attribution-NonDerivative-NonCommercial License, permitting copying and reproduction so long as the original work is given appropriate credit. Contents may not be used for commercial purposes, or adapted, remixed, transformed or built upon. ( https://creativecommons.org/licenses/by-nc-nd/4.0/ ).
Conflict of interest statement
Conflict of Interest None declared.
Figures




Similar articles
-
Pancreatic exocrine insufficiency: Comparing fecal elastase 1 with 72-h stool for fecal fat estimation.Indian J Gastroenterol. 2016 Nov;35(6):441-444. doi: 10.1007/s12664-016-0714-4. Epub 2016 Nov 23. Indian J Gastroenterol. 2016. PMID: 27878466
-
Comparison of two tubeless function tests in the assessment of mild-to-moderate exocrine pancreatic insufficiency.Eur J Gastroenterol Hepatol. 2000 Dec;12(12):1335-8. doi: 10.1097/00042737-200012120-00012. Eur J Gastroenterol Hepatol. 2000. PMID: 11192324 Clinical Trial.
-
The investigation and management of pancreatic exocrine insufficiency: A retrospective cohort study.Clin Med (Lond). 2020 Nov;20(6):535-540. doi: 10.7861/clinmed.2020-0506. Clin Med (Lond). 2020. PMID: 33199316 Free PMC article.
-
Potential for Screening for Pancreatic Exocrine Insufficiency Using the Fecal Elastase-1 Test.Dig Dis Sci. 2017 May;62(5):1119-1130. doi: 10.1007/s10620-017-4524-z. Epub 2017 Mar 17. Dig Dis Sci. 2017. PMID: 28315028 Review.
-
Staging exocrine pancreatic dysfunction.Pancreatology. 2022 Jan;22(1):168-172. doi: 10.1016/j.pan.2021.11.005. Epub 2021 Nov 19. Pancreatology. 2022. PMID: 34916141 Review.
Cited by
-
High Incidence and Impact of Suspected Exocrine Pancreatic Insufficiency in Patients Post-Hematopoietic Stem Cell Transplantation: A Single-Center Prospective Observational Study.United European Gastroenterol J. 2025 Mar;13(2):257-267. doi: 10.1002/ueg2.12769. Epub 2025 Feb 15. United European Gastroenterol J. 2025. PMID: 39955611 Free PMC article.
-
Association between severity of pancreatic exocrine insufficiency and computed tomography-based morphological severity in patients with chronic pancreatitis.Medicine (Baltimore). 2024 Nov 29;103(48):e40737. doi: 10.1097/MD.0000000000040737. Medicine (Baltimore). 2024. PMID: 39612393 Free PMC article.
References
-
- Beyer G, Habtezion A, Werner J, Lerch M M, Mayerle J.Chronic pancreatitis Lancet 2020396(10249):499–512. - PubMed
-
- Clain J E, Pearson R K. Diagnosis of chronic pancreatitis. Is a gold standard necessary? Surg Clin North Am. 1999;79(04):829–845. - PubMed
-
- de la Iglesia-Garcia D, Vallejo-Senra N, Iglesias-Garcia J, López-López A, Nieto L, Domínguez-Muñoz J E. Increased risk of mortality associated with pancreatic exocrine insufficiency in patients with chronic pancreatitis. J Clin Gastroenterol. 2018;52(08):e63–e72. - PubMed
-
- Domínguez-Muñoz J E. Pancreatic exocrine insufficiency: diagnosis and treatment. J Gastroenterol Hepatol. 2011;26 02:12–16. - PubMed
LinkOut - more resources
Full Text Sources