

Cocreating the ICU-PAUSE Tool for Intensive Care Unit-Ward Transitions
- PMID: 35924191
- PMCID: PMC9341494
- DOI: 10.34197/ats-scholar.2021-0135IN
Cocreating the ICU-PAUSE Tool for Intensive Care Unit-Ward Transitions
Abstract
Background: Intensive care unit (ICU)-ward patient transfers are inherently high risk, and clinician miscommunication has been linked to adverse events and negative outcomes. Despite these risks, few educational tools exist to improve resident handoff communication at ICU-ward transfer.
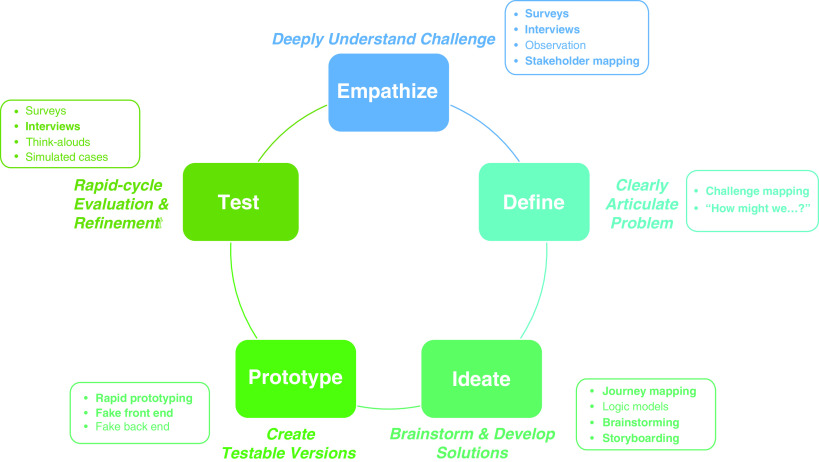
Objective: We used human-centered design (HCD) methods to cocreate a novel electronic health record ICU-ward transfer tool alongside Internal Medicine residents at three academic hospitals.
Methods: We conducted HCD workshops at each hospital, performing process mapping, brainstorming, and rapid prototyping. We performed thematic analysis on verbatim-transcribed workshop audio recordings to inform development and adaptation of the final resident prototype into the ICU-PAUSE tool.
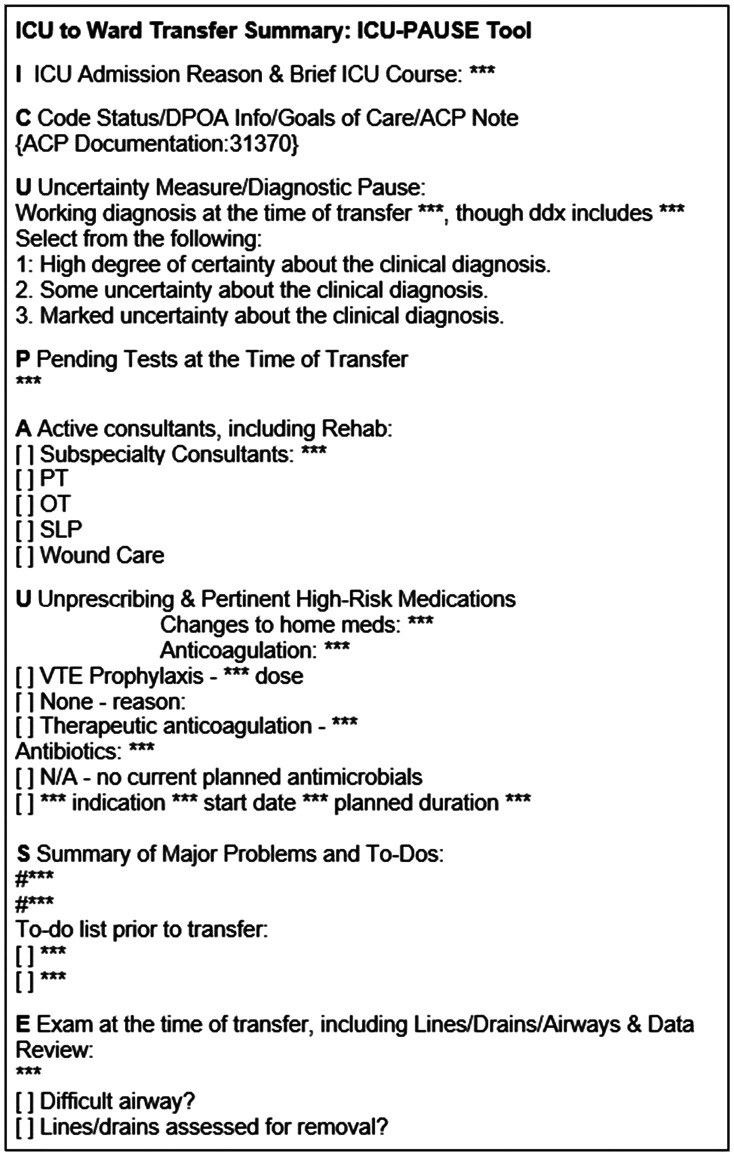
Results: ICU-PAUSE focuses on reasons for ICU admission and problem-based ICU course (I); Code status, goals of care, and family contacts (C); a diagnostic pause acknowledging Uncertainty (U); Pending tests (P); Active consultants (A); high-risk medications, including medications to be Unprescribed (U); Summary of problems and to-dos (S); and a current physical Exam (E).
Conclusion: We used HCD to cocreate a novel, more user-friendly electronic ICU-ward transfer tool, ICU-PAUSE, alongside Internal Medicine trainees. Future steps will involve formal usability testing, evidence-driven implementation, and clinical evaluation of ICU-PAUSE across multiple hospitals.
Keywords: handoffs; human-centered design; qualitative research methods; quality-improvement education; transitions of care.
Copyright © 2022 by the American Thoracic Society.
Figures
Similar articles
-
Improving Communication in Intensive Care Unit to Ward Transitions: Protocol for Multisite National Implementation of the ICU-PAUSE Handoff Tool.JMIR Res Protoc. 2023 Feb 6;12:e40918. doi: 10.2196/40918. JMIR Res Protoc. 2023. PMID: 36745494 Free PMC article.
-
Scaling up a diagnostic pause at the ICU-to-ward transition: an exploration of barriers and facilitators to implementation of the ICU-PAUSE handoff tool.Diagnosis (Berl). 2023 Aug 21;10(4):417-423. doi: 10.1515/dx-2023-0046. eCollection 2023 Nov 1. Diagnosis (Berl). 2023. PMID: 37598362
-
Characterising ICU-ward handoffs at three academic medical centres: process and perceptions.BMJ Qual Saf. 2019 Aug;28(8):627-634. doi: 10.1136/bmjqs-2018-008328. Epub 2019 Jan 12. BMJ Qual Saf. 2019. PMID: 30636201
-
Going back to the ward-transitioning care back to the ward team.Transl Pediatr. 2018 Oct;7(4):314-325. doi: 10.21037/tp.2018.08.01. Transl Pediatr. 2018. PMID: 30460184 Free PMC article. Review.
-
Improving Patient Safety in Handover From Intensive Care Unit to General Ward: A Systematic Review.J Patient Saf. 2020 Sep;16(3):199-210. doi: 10.1097/PTS.0000000000000266. J Patient Saf. 2020. PMID: 28452913
Cited by
-
Improving Communication in Intensive Care Unit to Ward Transitions: Protocol for Multisite National Implementation of the ICU-PAUSE Handoff Tool.JMIR Res Protoc. 2023 Feb 6;12:e40918. doi: 10.2196/40918. JMIR Res Protoc. 2023. PMID: 36745494 Free PMC article.
-
Redesigning the Hospital Environment to Improve Restfulness.JAMA Netw Open. 2024 Dec 2;7(12):e2447790. doi: 10.1001/jamanetworkopen.2024.47790. JAMA Netw Open. 2024. PMID: 39630451 Free PMC article.
-
Validating the Physician Documentation Quality Instrument for Intensive Care Unit-Ward Transfer Notes.ATS Sch. 2024 Feb 27;5(2):274-285. doi: 10.34197/ats-scholar.2023-0094OC. eCollection 2024 Jun 1. ATS Sch. 2024. PMID: 39055332 Free PMC article.
-
Receipt of Recovery-Oriented Care Practices During Hospitalization for Sepsis.Crit Care Explor. 2022 Sep 13;4(9):e0766. doi: 10.1097/CCE.0000000000000766. eCollection 2022 Sep. Crit Care Explor. 2022. PMID: 36119396 Free PMC article.
References
-
- Santhosh L, Lyons PG, Rojas JC, Ciesielski TM, Beach S, Farnan JM, et al. Characterising ICU-ward handoffs at three academic medical centres: process and perceptions. BMJ Qual Saf . 2019;28:627–634. - PubMed
-
- Starmer AJ, Spector ND, Srivastava R, West DC, Rosenbluth G, Allen AD, et al. I-PASS Study Group Changes in medical errors after implementation of a handoff program. N Engl J Med . 2014;371:1803–1812. - PubMed
