

The role of cardiac magnetic resonance imaging in the assessment of heart failure with preserved ejection fraction
- PMID: 35924215
- PMCID: PMC9339656
- DOI: 10.3389/fcvm.2022.922398
The role of cardiac magnetic resonance imaging in the assessment of heart failure with preserved ejection fraction
Abstract
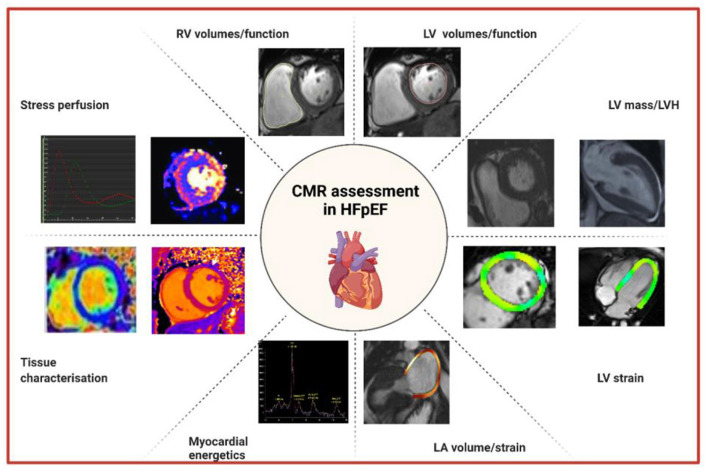
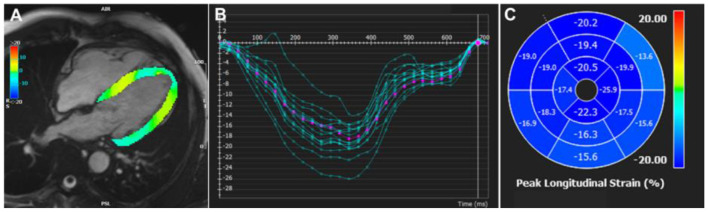
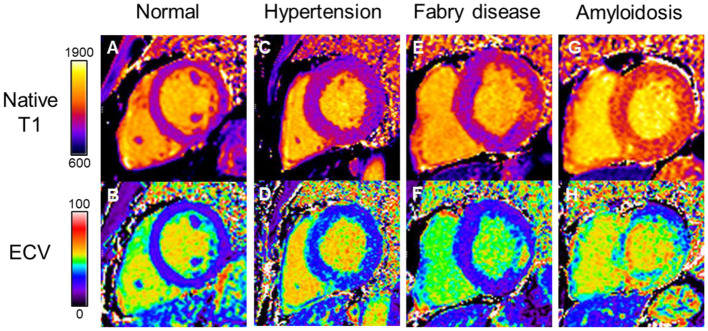
Heart failure (HF) is a major cause of morbidity and mortality worldwide. Current classifications of HF categorize patients with a left ventricular ejection fraction of 50% or greater as HF with preserved ejection fraction or HFpEF. Echocardiography is the first line imaging modality in assessing diastolic function given its practicality, low cost and the utilization of Doppler imaging. However, the last decade has seen cardiac magnetic resonance (CMR) emerge as a valuable test for the sometimes challenging diagnosis of HFpEF. The unique ability of CMR for myocardial tissue characterization coupled with high resolution imaging provides additional information to echocardiography that may help in phenotyping HFpEF and provide prognostication for patients with HF. The precision and accuracy of CMR underlies its use in clinical trials for the assessment of novel and repurposed drugs in HFpEF. Importantly, CMR has powerful diagnostic utility in differentiating acquired and inherited heart muscle diseases presenting as HFpEF such as Fabry disease and amyloidosis with specific treatment options to reverse or halt disease progression. This state of the art review will outline established CMR techniques such as transmitral velocities and strain imaging of the left ventricle and left atrium in assessing diastolic function and their clinical application to HFpEF. Furthermore, it will include a discussion on novel methods and future developments such as stress CMR and MR spectroscopy to assess myocardial energetics, which show promise in unraveling the mechanisms behind HFpEF that may provide targets for much needed therapeutic interventions.
Keywords: CMR in HFpEF; HFpEF; diastolic dysfunction; diastolic function; diastolic heart failure.
Copyright © 2022 Lau, Elshibly, Kanagala, Khoo, Arnold and Hothi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Exercise Stress Real-Time Cardiac Magnetic Resonance Imaging for Noninvasive Characterization of Heart Failure With Preserved Ejection Fraction: The HFpEF-Stress Trial.Circulation. 2021 Apr 13;143(15):1484-1498. doi: 10.1161/CIRCULATIONAHA.120.051542. Epub 2021 Jan 21. Circulation. 2021. PMID: 33472397
-
Cardiovascular magnetic resonance feature tracking for characterization of patients with heart failure with preserved ejection fraction: correlation of global longitudinal strain with invasive diastolic functional indices.J Cardiovasc Magn Reson. 2020 Jun 4;22(1):42. doi: 10.1186/s12968-020-00636-w. J Cardiovasc Magn Reson. 2020. PMID: 32498688 Free PMC article.
-
Heart failure with preserved ejection fraction assessed by cardiac magnetic resonance: From clinical uses to emerging techniques.Trends Cardiovasc Med. 2023 Apr;33(3):141-147. doi: 10.1016/j.tcm.2021.12.006. Epub 2021 Dec 18. Trends Cardiovasc Med. 2023. PMID: 34933114 Review.
-
Heart failure with preserved ejection fraction in post myocardial infarction patients: a myocardial magnetic resonance (MR) tissue tracking study.Quant Imaging Med Surg. 2023 Mar 1;13(3):1723-1739. doi: 10.21037/qims-22-793. Epub 2022 Dec 26. Quant Imaging Med Surg. 2023. PMID: 36915319 Free PMC article.
-
CMR to characterize myocardial structure and function in heart failure with preserved left ventricular ejection fraction.Eur Heart J Cardiovasc Imaging. 2024 Oct 30;25(11):1491-1504. doi: 10.1093/ehjci/jeae224. Eur Heart J Cardiovasc Imaging. 2024. PMID: 39205602 Free PMC article. Review.
Cited by
-
Cardiac Magnetic Resonance Left Ventricular Filling Pressure Is Associated with NT-proBNP in Patients with New Onset Heart Failure.Medicina (Kaunas). 2023 Oct 30;59(11):1924. doi: 10.3390/medicina59111924. Medicina (Kaunas). 2023. PMID: 38003973 Free PMC article.
-
Predictors of prognosis by cardiac magnetic resonance imaging in patients with idiopathic restrictive heart disease.Egypt Heart J. 2025 Jun 16;77(1):63. doi: 10.1186/s43044-025-00657-9. Egypt Heart J. 2025. PMID: 40522548 Free PMC article.
-
Assessment of Microvascular Disease in Heart and Brain by MRI: Application in Heart Failure with Preserved Ejection Fraction and Cerebral Small Vessel Disease.Medicina (Kaunas). 2023 Sep 4;59(9):1596. doi: 10.3390/medicina59091596. Medicina (Kaunas). 2023. PMID: 37763715 Free PMC article. Review.
-
Cardiac MRI in heart failure with preserved ejection fraction.Radiol Med. 2024 Oct;129(10):1468-1484. doi: 10.1007/s11547-024-01874-z. Epub 2024 Aug 19. Radiol Med. 2024. PMID: 39158816 Review.
-
Heart Failure with Preserved Ejection Fraction Correlates with Fibrotic Atrial Myopathy in Patients Undergoing Atrial Fibrillation Ablation.J Clin Med. 2024 Sep 24;13(19):5685. doi: 10.3390/jcm13195685. J Clin Med. 2024. PMID: 39407745 Free PMC article.
References
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. . Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1789–858. 10.1016/S0140-6736(18)32279-7 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous