

Isolated knee extensor exercise training improves skeletal muscle vasodilation, blood flow, and functional capacity in patients with HFpEF
- PMID: 35924338
- PMCID: PMC9350466
- DOI: 10.14814/phy2.15419
Isolated knee extensor exercise training improves skeletal muscle vasodilation, blood flow, and functional capacity in patients with HFpEF
Abstract
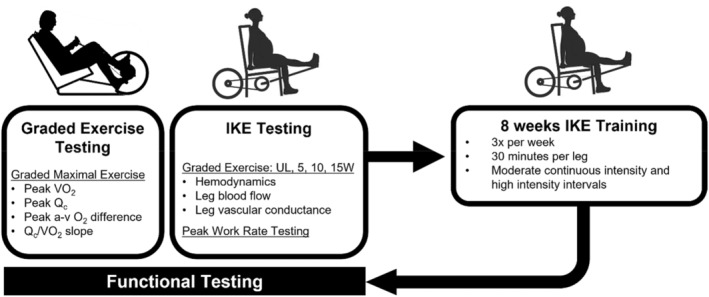
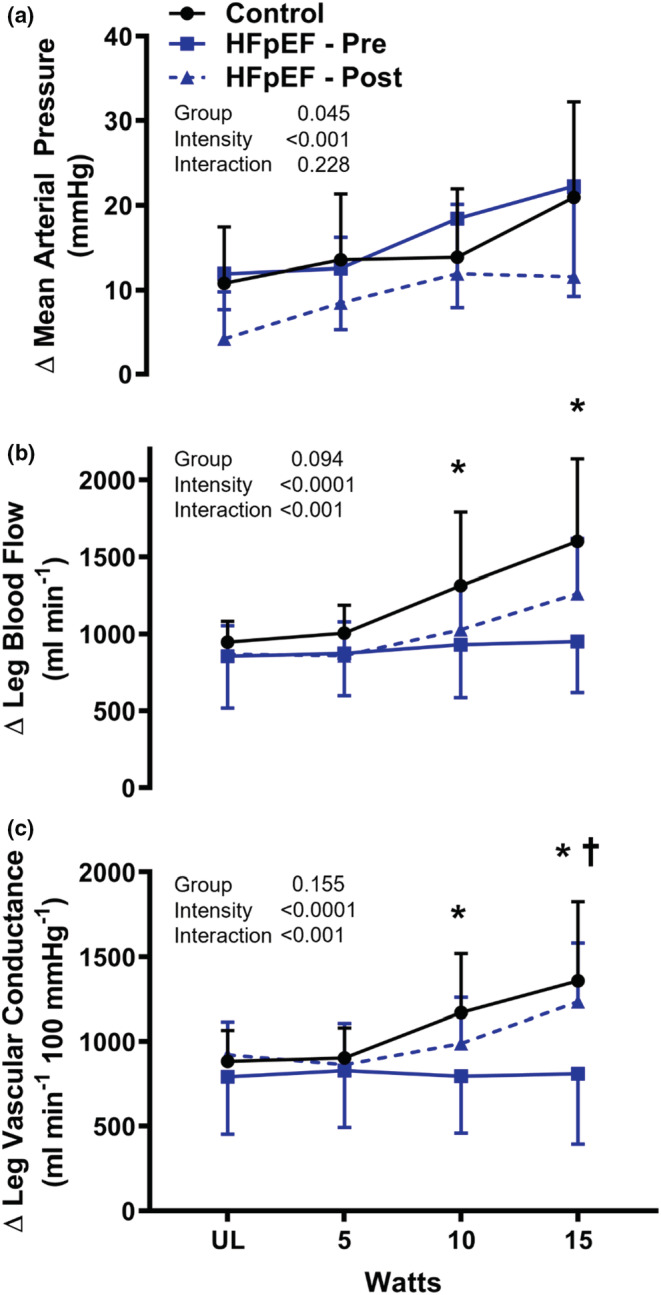
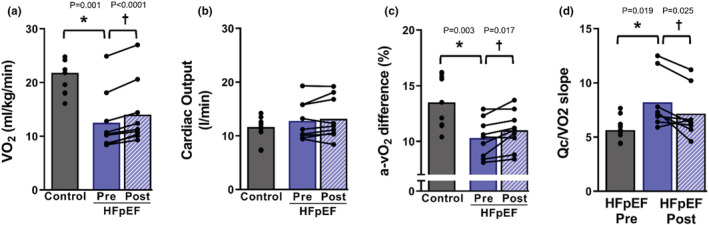
Patients with HFpEF experience severe exercise intolerance due in part to peripheral vascular and skeletal muscle impairments. Interventions targeting peripheral adaptations to exercise training may reverse vascular dysfunction, increase peripheral oxidative capacity, and improve functional capacity in HFpEF. Determine if 8 weeks of isolated knee extension exercise (KE) training will reverse vascular dysfunction, peripheral oxygen utilization, and exercise capacity in patients with HFpEF. Nine HFpEF patients (66 ± 5 years, 6 females) performed graded IKE exercise (5, 10, and 15 W) and maximal exercise testing (cycle ergometer) before and after IKE training (3x/week, 30 min/leg). Femoral blood flow (ultrasound) and leg vascular conductance (LVC; index of vasodilation) were measured during graded IKE exercise. Peak pulmonary oxygen uptake (V̇O2 ; Douglas bags) and cardiac output (QC ; acetylene rebreathe) were measured during graded maximal cycle exercise. IKE training improved LVC (pre: 810 ± 417, post: 1234 ± 347 ml/min/100 mmHg; p = 0.01) during 15 W IKE exercise and increased functional capacity by 13% (peak V̇O2 during cycle ergometry; pre:12.4 ± 5.2, post: 14.0 ± 6.0 ml/min/kg; p = 0.01). The improvement in peak V̇O2 was independent of changes in Q̇c (pre:12.7 ± 3.5, post: 13.2 ± 3.9 L/min; p = 0.26) and due primarily to increased a-vO2 difference (pre: 10.3 ± 1.6, post: 11.0 ± 1.7; p = 0.02). IKE training improved vasodilation and functional capacity in patients with HFpEF. Exercise interventions aimed at increasing peripheral oxidative capacity may be effective therapeutic options for HFpEF patients.
© 2022 The Authors. Physiological Reports published by Wiley Periodicals LLC on behalf of The Physiological Society and the American Physiological Society.
Conflict of interest statement
All data are available upon reasonable request. The authors have no competing interests. Experiments were performed at the Institute for Exercise and Environmental Medicine.
Figures
Similar articles
-
Identifying the Mechanisms of a Peripherally Limited Exercise Phenotype in Patients With Heart Failure With Preserved Ejection Fraction.Circ Heart Fail. 2024 Aug;17(8):e011693. doi: 10.1161/CIRCHEARTFAILURE.123.011693. Epub 2024 Jul 25. Circ Heart Fail. 2024. PMID: 39051098 Free PMC article. Clinical Trial.
-
Heart-Lung Interactions in HFpEF: Dynamic Hyperinflation and Exercise PCWP.JACC Heart Fail. 2025 Aug;13(8):102523. doi: 10.1016/j.jchf.2025.102523. Epub 2025 Jun 26. JACC Heart Fail. 2025. PMID: 40578265 Clinical Trial.
-
α-Adrenergic regulation of skeletal muscle blood flow during exercise in patients with heart failure with preserved ejection fraction.J Physiol. 2024 Jul;602(14):3401-3422. doi: 10.1113/JP285526. Epub 2024 Jun 6. J Physiol. 2024. PMID: 38843407 Free PMC article.
-
Sex-based differences in peak oxygen uptake among individuals with heart failure: systematic review and meta-analysis.J Appl Physiol (1985). 2025 Jul 1;139(1):45-57. doi: 10.1152/japplphysiol.00153.2025. Epub 2025 Jun 4. J Appl Physiol (1985). 2025. PMID: 40465477
-
Physiological determinants of decreased peak leg oxygen uptake in chronic disease: a systematic review and meta-analysis.J Appl Physiol (1985). 2024 Jun 1;136(6):1293-1302. doi: 10.1152/japplphysiol.00918.2023. Epub 2024 Mar 14. J Appl Physiol (1985). 2024. PMID: 38482572
Cited by
-
The Oxygen Cascade According to HFpEF Likelihood: A Focus on Sex Differences.JACC Adv. 2024 Jun 11;3(7):101039. doi: 10.1016/j.jacadv.2024.101039. eCollection 2024 Jul. JACC Adv. 2024. PMID: 39130052 Free PMC article.
-
Characterization of a novel ovine model of hypertensive heart failure with preserved ejection fraction.Am J Physiol Heart Circ Physiol. 2024 Dec 1;327(6):H1490-H1502. doi: 10.1152/ajpheart.00548.2024. Epub 2024 Nov 15. Am J Physiol Heart Circ Physiol. 2024. PMID: 39546298 Free PMC article.
-
Identifying the Mechanisms of a Peripherally Limited Exercise Phenotype in Patients With Heart Failure With Preserved Ejection Fraction.Circ Heart Fail. 2024 Aug;17(8):e011693. doi: 10.1161/CIRCHEARTFAILURE.123.011693. Epub 2024 Jul 25. Circ Heart Fail. 2024. PMID: 39051098 Free PMC article. Clinical Trial.
-
The sympathetic nervous system in heart failure with preserved ejection fraction.Heart Fail Rev. 2025 Jan;30(1):209-218. doi: 10.1007/s10741-024-10456-0. Epub 2024 Oct 23. Heart Fail Rev. 2025. PMID: 39438394 Free PMC article. Review.
-
Statin administration improves vascular function in heart failure with preserved ejection fraction.J Appl Physiol (1985). 2024 Apr 1;136(4):877-888. doi: 10.1152/japplphysiol.00775.2023. Epub 2024 Feb 22. J Appl Physiol (1985). 2024. PMID: 38385181 Free PMC article. Clinical Trial.
References
-
- Andersen, P. , Adams, R. P. , Sjøgaard, G. , Thorboe, A. , & Saltin, B. (1985). Dynamic knee extension as model for study of isolated exercising muscle in humans. Journal of Applied Physiology, 59(1647–1653), 1985–1653. - PubMed
-
- Balmain, S. , Padmanabhan, N. , Ferrell, W. R. , Morton, J. J. , & McMurray, J. J. (2007). Differences in arterial compliance, microvascular function and venous capacitance between patients with heart failure and either preserved or reduced left ventricular systolic function. European Journal of Heart Failure, 9, 865–871. - PubMed
-
- Bhella, P. S. , Prasad, A. , Heinicke, K. , Hastings, J. L. , Arbab‐Zadeh, A. , Adams‐Huet, B. , Pacini, E. L. , Shibata, S. , Palmer, M. D. , Newcomer, B. R. , & Levine, B. D. (2011). Abnormal haemodynamic response to exercise in heart failure with preserved ejection fraction. European Journal of Heart Failure, 13, 1296–1304. - PMC - PubMed
-
- Borlaug, B. A. , Melenovsky, V. , Russell, S. D. , Kessler, K. , Pacak, K. , Becker, L. C. , & Kass, D. A. (2006). Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation, 114, 2138–2147. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
