

De Novo dural arteriovenous fistulas after endovascular treatment: Case illustration and literature review
- PMID: 35924383
- PMCID: PMC11475303
- DOI: 10.1177/15910199221118517
De Novo dural arteriovenous fistulas after endovascular treatment: Case illustration and literature review
Abstract
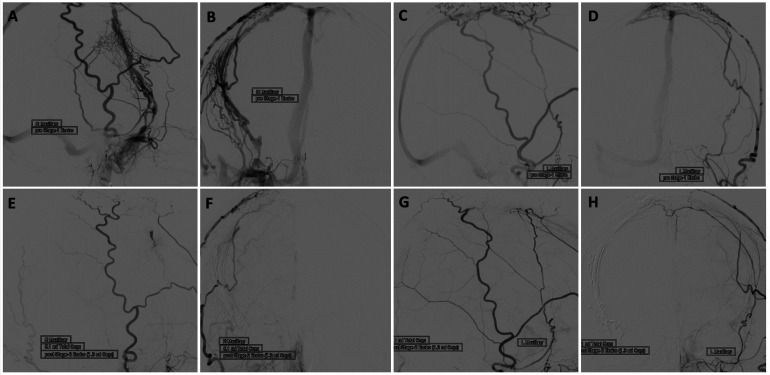
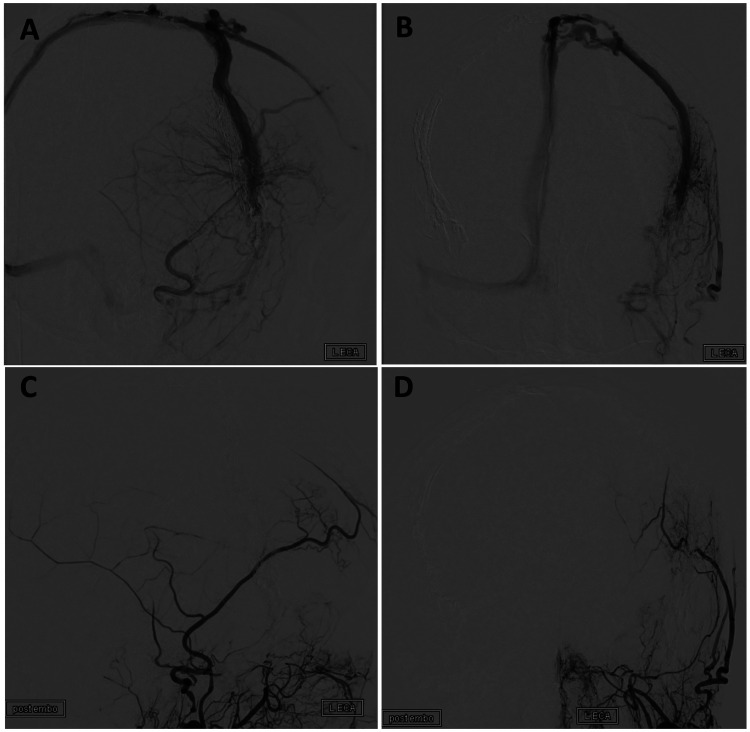
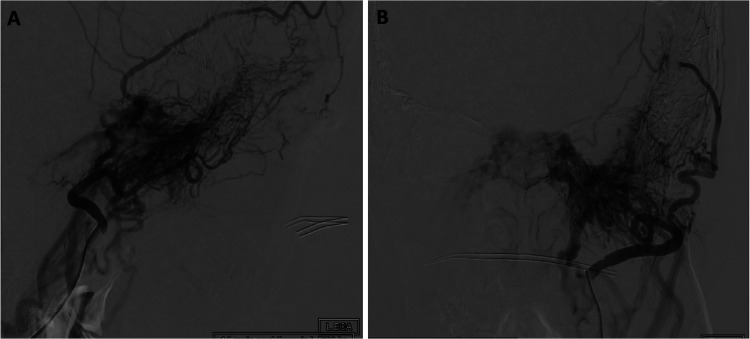
Intracranial dural arteriovenous fistulas (dAVF) account for nearly 10-15% of all arteriovenous malformations. Although the majority of dAVF are effectively cured after endovascular intervention, there are cases of dAVFs that may recur after radiographic cure. We present the case of a 69-year-old female with de novo formation of three dAVFs in different anatomic locations after successive endovascular treatments. The patient's initial dAVF was identified in the right posterior frontal convexity region and obliterated with transarterial and transvenous embolization. The patient returned eight years later due to left-sided pulsatile tinnitus and a new dAVF in the left greater sphenoid wing region was seen on angiography. This was treated with transvenous embolization with complete resolution. One year later, she developed left sided pulsatile tinnitus again and was found to have a left carotid-cavernous dAVF. This is the first case report to our knowledge of the formation of three de novo dAVFs over multiple years in distinct anatomical locations. We also review the literature regarding de novo dAVFs after endovascular treatment which includes 16 cases. De novo dAVF formation is likely due to numerous factors including changes in venous flow and aberrant vascular development. It is important to further understand the relationship between endovascular treatment and recurrent dAVF formation to prevent subsequent malformations.
Keywords: de novo formation; dural arteriovenous fistula; endovascular treatment; liquid embolic.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
Parasagittal and Superior Sagittal Sinus Dural Arteriovenous Fistulas: Clinical Presentations, Imaging Characteristics, and Treatment Strategies.AJNR Am J Neuroradiol. 2024 Aug 9;45(8):1025-1030. doi: 10.3174/ajnr.A8246. AJNR Am J Neuroradiol. 2024. PMID: 38479780 Free PMC article.
-
Dural arteriovenous fistulas of the hypoglossal canal: systematic review on imaging anatomy, clinical findings, and endovascular management.J Neurosurg. 2015 Apr;122(4):883-903. doi: 10.3171/2014.10.JNS14377. Epub 2014 Nov 21. J Neurosurg. 2015. PMID: 25415064
-
Endovascular treatment of intracranial dural arteriovenous fistulas with Onyx: A consecutive series of 62 patients from a single-center.Neuroradiol J. 2024 Oct;37(5):587-592. doi: 10.1177/19714009241242586. Epub 2024 Apr 1. Neuroradiol J. 2024. PMID: 38557275
-
Transvenous approach: a promising strategy for endovascular treatment of cribriform plate dural arteriovenous fistula.J Neurosurg. 2025 Apr 4;143(2):505-511. doi: 10.3171/2024.12.JNS241501. Print 2025 Aug 1. J Neurosurg. 2025. PMID: 40184685
-
Feasibility, safety, and efficacy of endovascular treatment of anterior cranial fossa dural arteriovenous fistulas: a systematic review and meta-analysis with a subanalysis for Onyx.Neurosurg Rev. 2024 May 13;47(1):217. doi: 10.1007/s10143-024-02446-5. Neurosurg Rev. 2024. PMID: 38736006
Cited by
-
New insight into DAVF pathology-Clues from meningeal immunity.Front Immunol. 2022 Sep 15;13:858924. doi: 10.3389/fimmu.2022.858924. eCollection 2022. Front Immunol. 2022. PMID: 36189220 Free PMC article. Review.
-
Low- and Intermediate-Grade Lateral Sinus Dural Arteriovenous Fistulas: Factors Affecting the Outcome of Endovascular Treatment over 18-Year Experience in a High-Volume Neurovascular Center.AJNR Am J Neuroradiol. 2025 Jun 3;46(6):1152-1158. doi: 10.3174/ajnr.A8622. AJNR Am J Neuroradiol. 2025. PMID: 39672601
-
Dural arteriovenous fistula may be occluded through recanalization of impaired venous sinuses.Medicine (Baltimore). 2024 Oct 11;103(41):e40097. doi: 10.1097/MD.0000000000040097. Medicine (Baltimore). 2024. PMID: 39465811 Free PMC article.
References
-
- Newton TH, Cronqvist S. Involvement of dural arteries in intracranial arteriovenous malformations. Radiology 1969; 93: 1071–1078. - PubMed
-
- Gemmete JJ, Chaudhary N, Pandey A, et al. Treatment of carotid cavernous fistulas. Curr Treat Options Neurol 2010; 12: 43–53. - PubMed
-
- Fujita A, Nakamura M, Tamaki N. Multiple dural arteriovenous fistulas involving both the cavernous sinus and the posterior fossa: report of two cases and review of the literature. No Shinkei Geka Neurological Surgery 2001; 29: 1065–1072. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
