

Trends in survival after cardiac arrest: a Swedish nationwide study over 30 years
- PMID: 35924401
- PMCID: PMC9726448
- DOI: 10.1093/eurheartj/ehac414
Trends in survival after cardiac arrest: a Swedish nationwide study over 30 years
Abstract
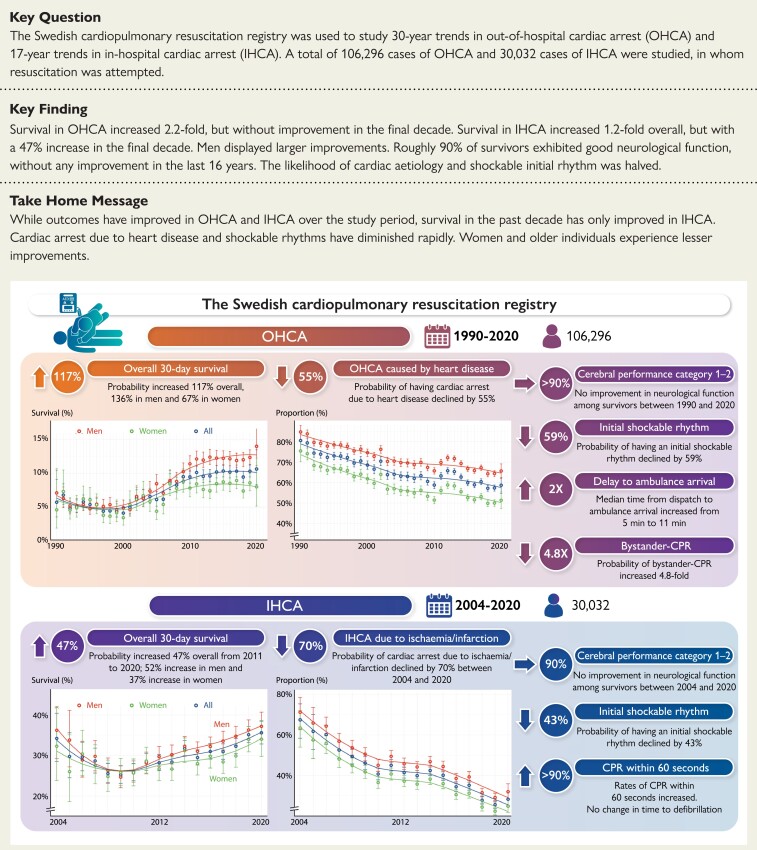
Aims: Trends in characteristics, management, and survival in out-of-hospital cardiac arrest (OHCA) and in-hospital cardiac arrest (IHCA) were studied in the Swedish Cardiopulmonary Resuscitation Registry (SCRR).
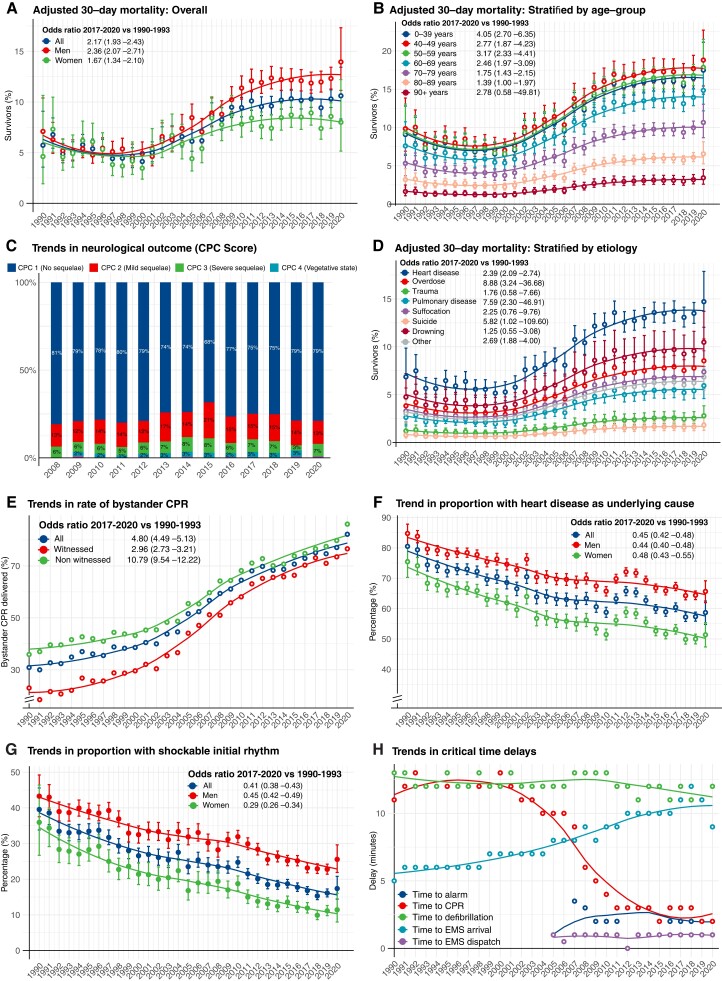
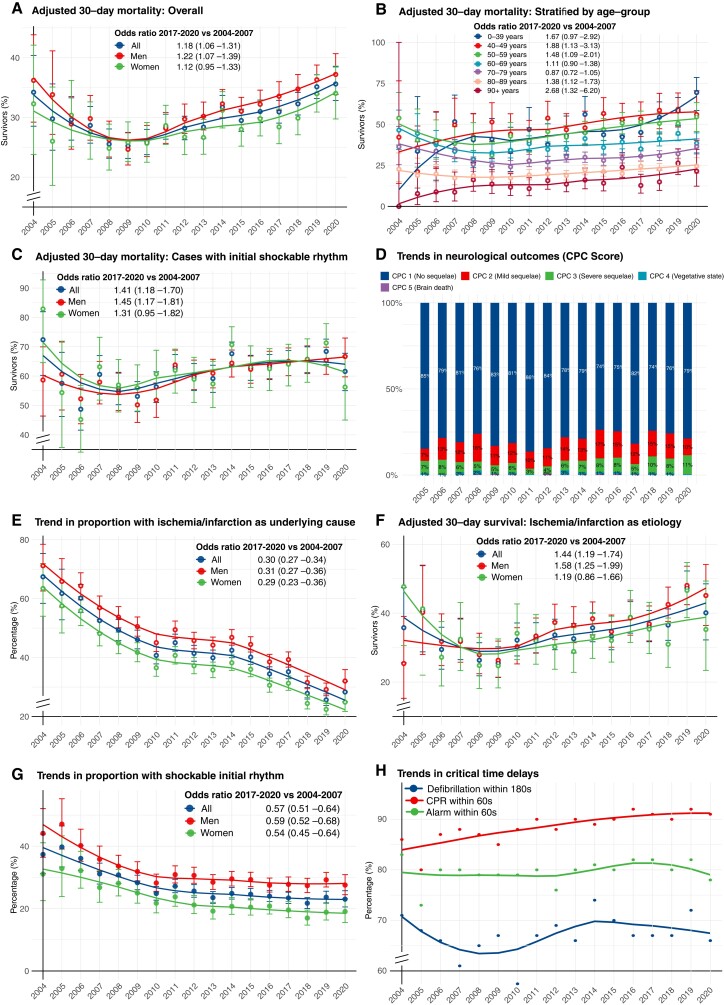
Methods and results: The SCRR was used to study 106 296 cases of OHCA (1990-2020) and 30 032 cases of IHCA (2004-20) in whom resuscitation was attempted. In OHCA, survival increased from 5.7% in 1990 to 10.1% in 2011 and remained unchanged thereafter. Odds ratios [ORs, 95% confidence interval (CI)] for survival in 2017-20 vs. 1990-93 were 2.17 (1.93-2.43) overall, 2.36 (2.07-2.71) for men, and 1.67 (1.34-2.10) for women. Survival increased for all aetiologies, except trauma, suffocation, and drowning. OR for cardiac aetiology in 2017-20 vs. 1990-93 was 0.45 (0.42-0.48). Bystander cardiopulmonary resuscitation increased from 30.9% to 82.2%. Shockable rhythm decreased from 39.5% in 1990 to 17.4% in 2020. Use of targeted temperature management decreased from 42.1% (2010) to 18.2% (2020). In IHCA, OR for survival in 2017-20 vs. 2004-07 was 1.18 (1.06-1.31), showing a non-linear trend with probability of survival increasing by 46.6% during 2011-20. Myocardial ischaemia or infarction as aetiology decreased during 2004-20 from 67.4% to 28.3% [OR 0.30 (0.27-0.34)]. Shockable rhythm decreased from 37.4% to 23.0% [OR 0.57 (0.51-0.64)]. Approximately 90% of survivors (IHCA and OHCA) had no or mild neurological sequelae.
Conclusion: Survival increased 2.2-fold in OHCA during 1990-2020 but without any improvement in the final decade, and 1.2-fold in IHCA during 2004-20, with rapid improvement the last decade. Cardiac aetiology and shockable rhythms were halved. Neurological outcome has not improved.
Keywords: Cardiac arrest; Cardiovascular disease; Heart disease; Resuscitation.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Cardiology.
Conflict of interest statement
Conflict of interest: none declared.
Figures
Comment in
-
The flatlining of cardiac arrest survival: can we revive the upward trend?Eur Heart J. 2022 Dec 7;43(46):4830-4831. doi: 10.1093/eurheartj/ehac522. Eur Heart J. 2022. PMID: 36269628 No abstract available.
References
-
- Gräsner J-T, Herlitz J, Tjelmeland IBM, Wnent J, Masterson S, Lilja Get al. European Resuscitation Council guidelines 2021: epidemiology of cardiac arrest in Europe. Resuscitation 2021;161:61–79. - PubMed
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson APet al. American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics 2020. Update: a report from the American Heart Association. Circulation 2020;141:e139–e596. - PubMed
-
- Hasselqvist-Ax I, Riva G, Herlitz J, Rosenqvist M, Hollenberg J, Nordberg Pet al. Early cardiopulmonary resuscitation in out-of-hospital cardiac arrest. N Engl J Med 2015;372:2307–2315. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
