

Current understanding of tandem spinal stenosis: epidemiology, diagnosis, and surgical strategy
- PMID: 35924651
- PMCID: PMC9458946
- DOI: 10.1530/EOR-22-0016
Current understanding of tandem spinal stenosis: epidemiology, diagnosis, and surgical strategy
Abstract
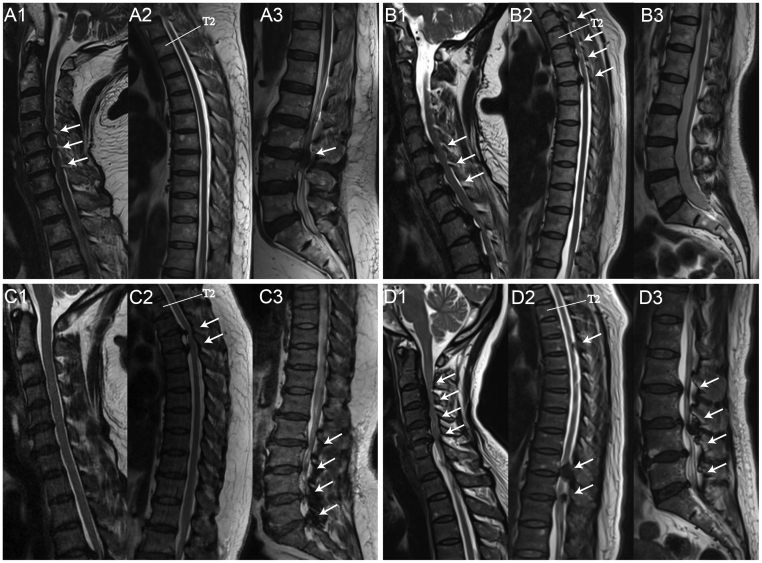
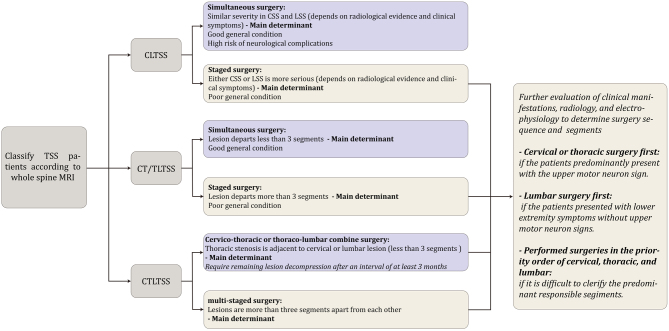
Tandem spinal stenosis (TSS) is defined as the concomitant occurrence of stenosis in at least two or more distinct regions (cervical, thoracic, or lumbar) of the spine and may present with a constellation of signs and symptoms. It has four subtypes, including cervico-lumbar, cervico-thoracic, thoraco-lumbar, and cervico-thoraco-lumbar TSS. The prevalence of TSS varies depending on the different subtypes and cohorts. The main aetiologies of TSS are spinal degenerative changes and heterotopic ossification, and patients with developmental spinal stenosis, ligament ossification, and spinal stenosis at any region are at an increased risk of developing TSS. The diagnosis of TSS is challenging. The clinical presentation of TSS could be complex, concealed, or severe, and these features may be confusing to clinicians, resulting in an incomplete or delayed diagnosis. Additionally, a consolidated diagnostic criterion for TSS is urgently required to improve consistency across studies and form a basis for establishing treatment guidelines. The optimal treatment option for TSS is still under debate; areas of controversies include choice of the decompression range, choice between simultaneous or staged surgical patterns, and the order of the surgeries. The present study reviews publications on TSS, consolidates current awareness on prevalence, aetiologies, potential risk factors, diagnostic dilemmas and criteria, and surgical strategies based on TSS subtypes. This is the first review to include thoracic spinal stenosis as a candidate disorder in TSS and aims at providing the readers with a comprehensive overview of TSS.
Keywords: diagnosis criteria; surgery; tandem spinal stenosis.
Figures
Similar articles
-
Development of a comprehensive treatment algorithm for tandem spinal stenosis: decision making and surgical strategy.Spine J. 2025 May 8:S1529-9430(25)00248-7. doi: 10.1016/j.spinee.2025.05.021. Online ahead of print. Spine J. 2025. PMID: 40348283
-
Delayed Diagnosis of Tandem Spinal Stenosis: A Retrospective Institutional Review.Int J Spine Surg. 2019 Jun 30;13(3):283-288. doi: 10.14444/6038. eCollection 2019 Jun. Int J Spine Surg. 2019. PMID: 31328093 Free PMC article.
-
Tandem stenosis of the cervical and thoracic spine: a systematic review.BMC Musculoskelet Disord. 2024 Aug 14;25(1):640. doi: 10.1186/s12891-024-07718-1. BMC Musculoskelet Disord. 2024. PMID: 39143570 Free PMC article.
-
Meta-Analysis of Simultaneous versus Staged Decompression of Stenotic Regions in Patients with Tandem Spinal Stenosis.World Neurosurg. 2023 Feb;170:e441-e454. doi: 10.1016/j.wneu.2022.11.028. Epub 2022 Nov 14. World Neurosurg. 2023. PMID: 36396060
-
Surgical outcomes for lumbar spinal canal stenosis with coexisting cervical stenosis (tandem spinal stenosis): a retrospective analysis of 565 cases.J Orthop Surg Res. 2018 Mar 20;13(1):60. doi: 10.1186/s13018-018-0765-6. J Orthop Surg Res. 2018. PMID: 29558952 Free PMC article.
Cited by
-
Evidence for a genetic contribution to the ossification of spinal ligaments in Ossification of Posterior Longitudinal Ligament and Diffuse idiopathic skeletal hyperostosis: A narrative review.Front Genet. 2022 Oct 7;13:987867. doi: 10.3389/fgene.2022.987867. eCollection 2022. Front Genet. 2022. PMID: 36276944 Free PMC article. Review.
-
Demographic and Clinical Characteristics of Patients With Cervical Spine Degeneration Reveal Frequent Cervicolumbar Tandem Spinal Stenosis in Mexico.Int J Spine Surg. 2023 Oct;17(5):670-677. doi: 10.14444/8520. Epub 2023 Jul 17. Int J Spine Surg. 2023. PMID: 37460237 Free PMC article.
-
Non-surgical treatment for tandem spinal stenosis: a systematic review protocol.BMJ Open. 2024 Nov 18;14(11):e084306. doi: 10.1136/bmjopen-2024-084306. BMJ Open. 2024. PMID: 39557546 Free PMC article.
-
Efficacy of measuring lysophosphatidylcholine levels in human cerebrospinal fluid to differentiate myelopathy from cauda equina syndrome.Sci Rep. 2025 Jul 8;15(1):24524. doi: 10.1038/s41598-025-08715-7. Sci Rep. 2025. PMID: 40628853 Free PMC article.
-
Accuracy and Reliability of Physical Signs as a Diagnostic Tool for Cervical Cord Compression: A Cross-Sectional Study.Spine Surg Relat Res. 2024 Oct 29;9(2):157-163. doi: 10.22603/ssrr.2024-0187. eCollection 2025 Mar 27. Spine Surg Relat Res. 2024. PMID: 40223840 Free PMC article.
References
-
- OSCIS investigators, Chikuda H, Koyama Y, Matsubayashi Y, Ogata T, Ohtsu H, Sugita S, Sumitani M, Kadono Y, Miura T, et al.Effect of early vs delayed surgical treatment on motor recovery in incomplete cervical spinal cord injury with preexisting cervical stenosis: a randomized clinical trial. JAMA Network Open 20214 e2133604. (10.1001/jamanetworkopen.2021.33604) - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
