

Brain topography on adult ultrasound images: Techniques, interpretation, and image library
- PMID: 35924877
- PMCID: PMC9804536
- DOI: 10.1111/jon.13031
Brain topography on adult ultrasound images: Techniques, interpretation, and image library
Abstract
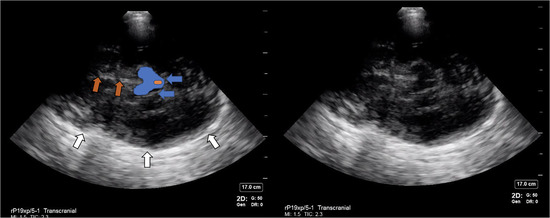
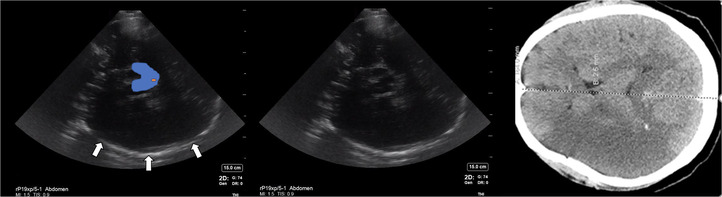
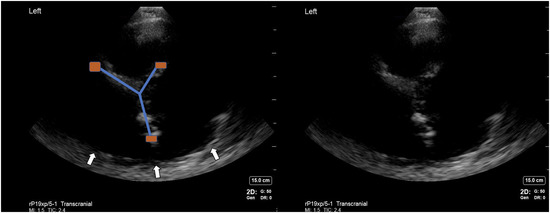
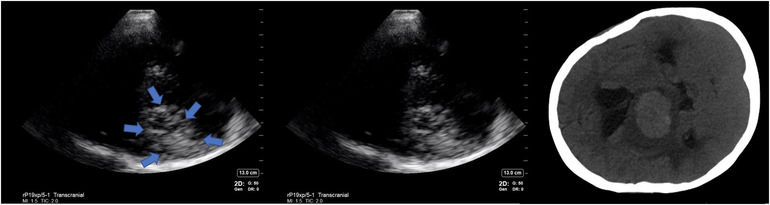
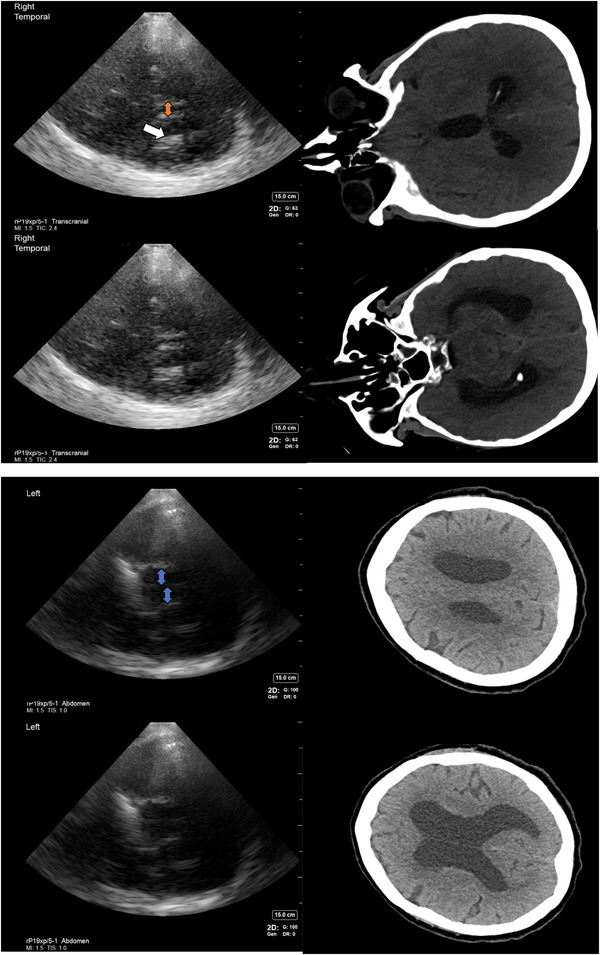
Background and purpose: Many studies have explored the possibility of using cranial ultrasound for discerning intracranial pathologies like tumors, hemorrhagic stroke, or subdural hemorrhage in clinical scenarios where computer tomography may not be accessible or feasible. The visualization of intracranial anatomy on B-mode ultrasound is challenging due to the presence of the skull that limits insonation to a few segments on the temporal bone that are thin enough to allow transcranial transmission of sound. Several artifacts are produced by hyperechoic signals inherent in brain and skull anatomy when images are created using temporal windows.
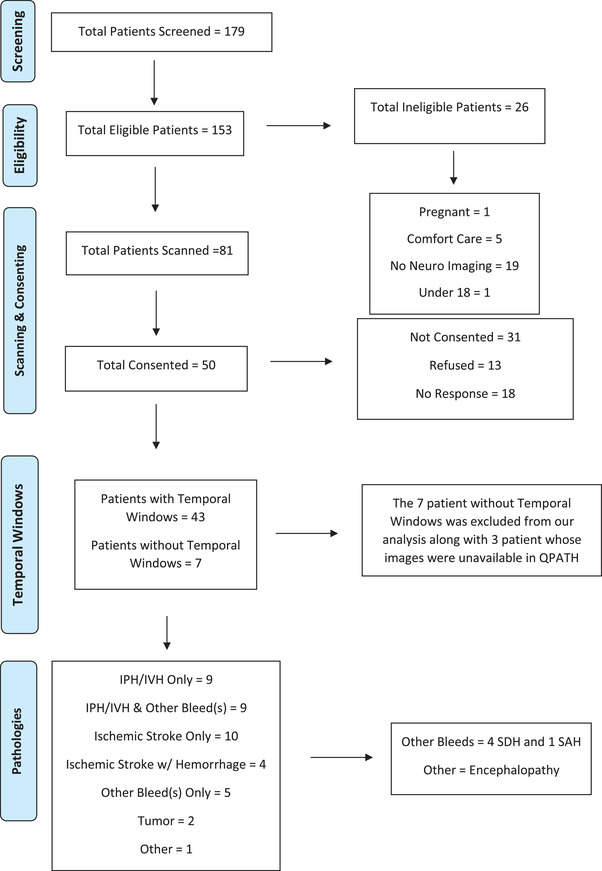
Methods: While the literature has investigated the accuracy of diagnosis of intracranial pathology with ultrasound, we lack a reference source for images acquired on cranial topography on B-mode ultrasound to illustrate the appearance of normal and abnormal structures of the brain and skull. Two investigators underwent hands-on training in Cranial point-of-care ultrasound (c-POCUS) and acquired multiple images from each patient to obtain the most in-depth images of brain to investigate all visible anatomical structures and pathology within 24 hours of any CT/MRI imaging done.
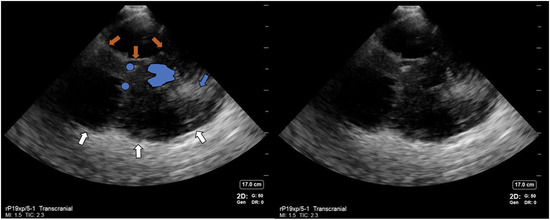
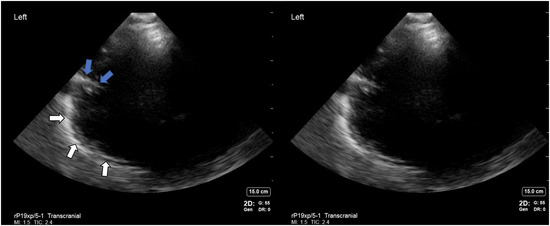
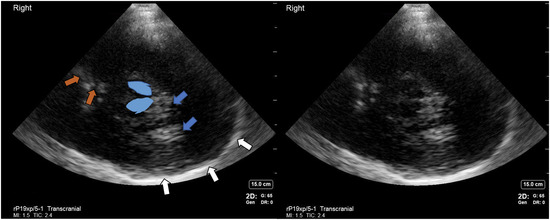
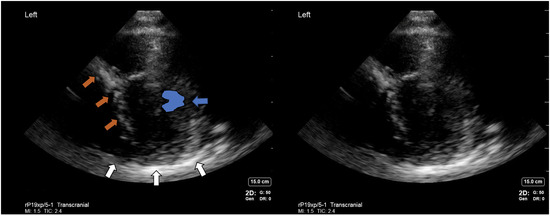
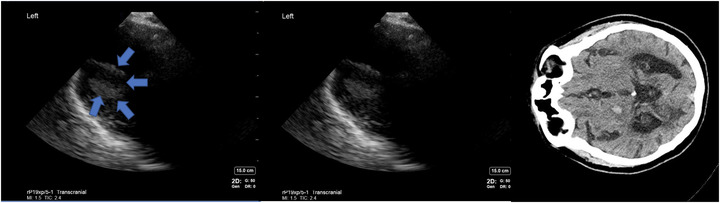
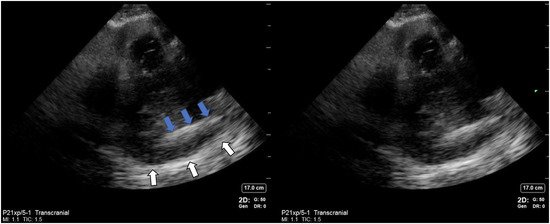
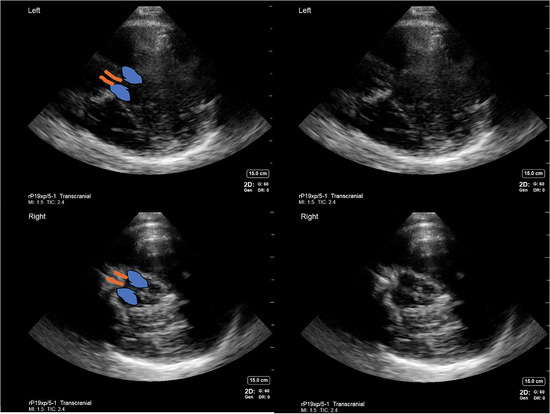
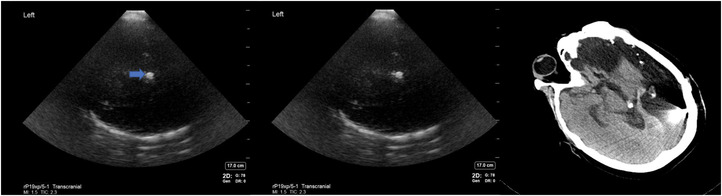
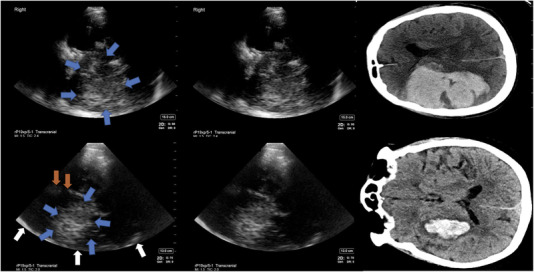
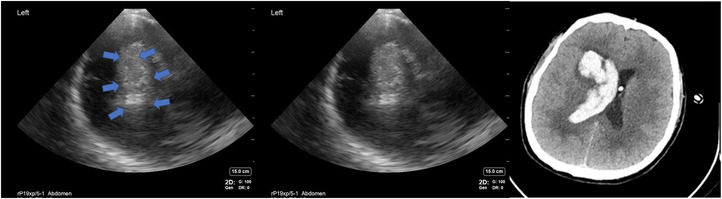
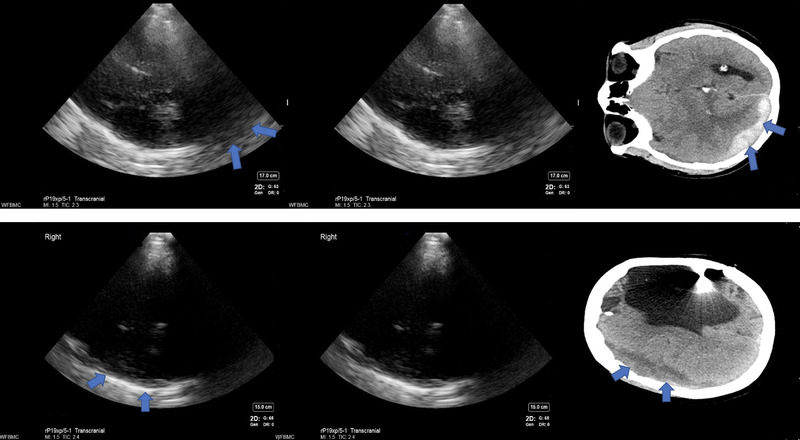
Results: Most reproducible structures visible on c-POCUS included bony parts and parenchymal structures. Transcranial and abdominal presets were equivalent in elucidating anatomical structures. Brain pathology like parenchymal hemorrhage, cerebral edema, and hydrocephalus were also visualized.
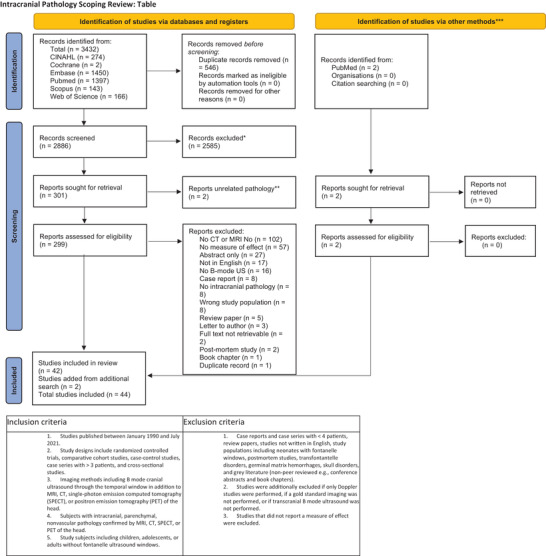
Conclusions: We present an illustrated anatomical atlas of cranial ultrasound B-mode images acquired in various pathologies in a critical care environment and compare our findings with published literature by performing a scoping review of literature on the subject.
Keywords: brain echography; cranial ultrasound; neuro-ultrasound; ultrasonography.
© 2022 The Authors. Journal of Neuroimaging published by Wiley Periodicals LLC on behalf of American Society of Neuroimaging.
Figures
References
-
- Alonso‐Canovas A, Lopez‐Sendon Moreno JL, Buisan J, et al. Does normal substantia nigra echogenicity make a difference in Parkinson's disease diagnosis? A real clinical practice follow‐up study. J Neurol 2018;265:2363–9. - PubMed
-
- Bor‐Seng‐Shu E, Pedroso JL, Felicio AC, et al. Substantia nigra echogenicity and imaging of striatal dopamine transporters in Parkinson's disease: a cross‐sectional study. Parkinsonism and Relat Disord 2014;20:477–81. - PubMed
-
- Iranzo A, Lomeña F, Stockner H, et al. Decreased striatal dopamine transporter uptake and substantia nigra hyperechogenicity as risk markers of synucleinopathy in patients with idiopathic rapid‐eye‐movement sleep behaviour disorder: a prospective study. Lancet Neurol 2010;9:1070–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
