

Diagnostic and Management Strategies in Patients with Late Recurrent Angina after Coronary Artery Bypass Grafting
- PMID: 35925511
- PMCID: PMC9556385
- DOI: 10.1007/s11886-022-01746-w
Diagnostic and Management Strategies in Patients with Late Recurrent Angina after Coronary Artery Bypass Grafting
Abstract
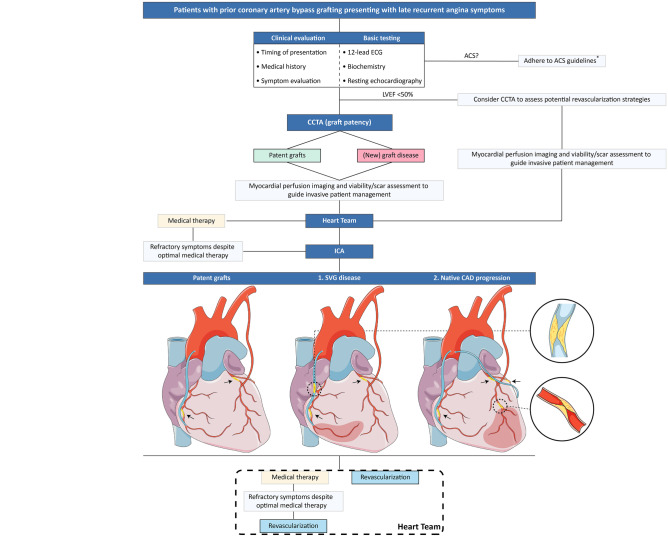
Purpose of review: This review will outline the current evidence on the anatomical, functional, and physiological tools that may be applied in the evaluation of patients with late recurrent angina after coronary artery bypass grafting (CABG). Furthermore, we discuss management strategies and propose an algorithm to guide decision-making for this complex patient population.
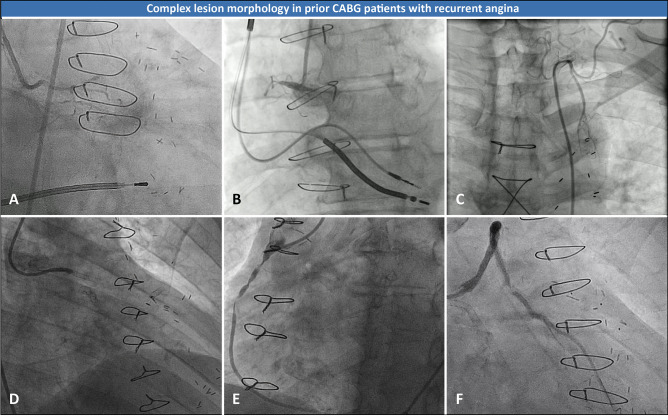
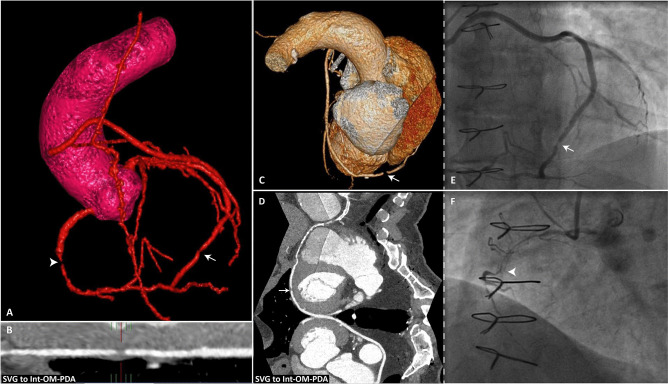
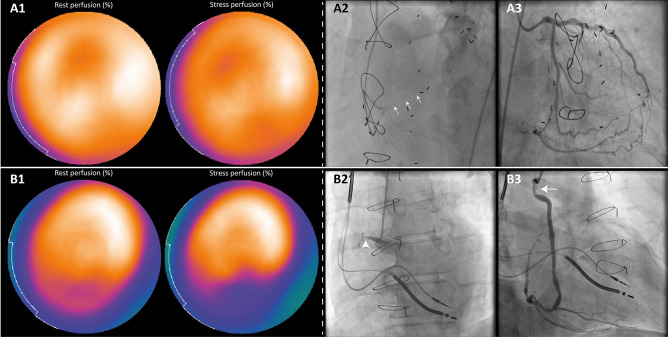
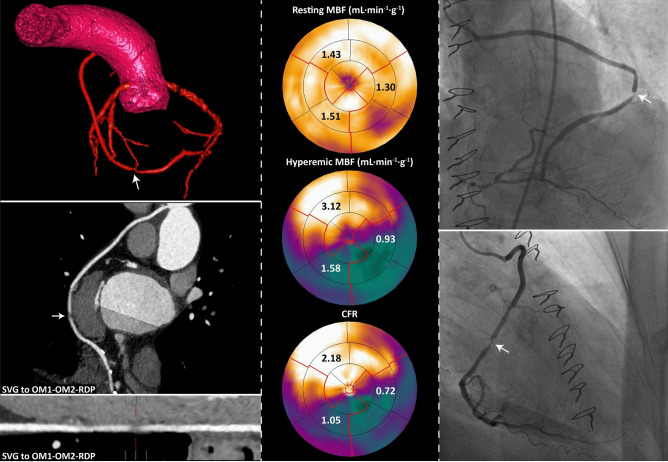
Recent findings: Patients with prior CABG often present with late recurrent angina as a result of bypass graft failure and progression of native coronary artery disease (CAD). These patients are generally older, have a higher prevalence of comorbidities, and more complex atherosclerotic lesion morphology compared to CABG-naïve patients. In addition, guideline recommendations are based on studies in which post-CABG patients have been largely excluded. Several invasive and non-invasive diagnostic tools are currently available to assess graft patency, the hemodynamic significance of native CAD progression, left ventricular function, and myocardial viability. Such tools, in particular the latest generation coronary computed tomography angiography, are part of a systematic diagnostic work-up to guide optimal repeat revascularization strategy in patients presenting with late recurrent angina after CABG.
Keywords: Diagnostic algorithm; Late recurrent angina; Prior coronary artery bypass grafting; Repeat revascularization.
© 2022. The Author(s).
Conflict of interest statement
None declared.
Figures
References
-
- • Neumann F-J, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2018;40(2):87-165. Most recent myocardial revascularization guidelines. - PubMed
-
- • Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2021. Most recent myocardial revascularization guidelines. - PubMed
-
- Fearon WF, Zimmermann FM, De Bruyne B, et al. Fractional flow reserve-guided PCI as compared with coronary bypass surgery. N Engl J Med. 2021. - PubMed
-
- Morrison DA, Sethi G, Sacks J, et al. Percutaneous coronary intervention versus repeat bypass surgery for patients with medically refractory myocardial ischemia: AWESOME randomized trial and registry experience with post-CABG patients. J Am Coll Cardiol. 2002;40(11):1951–1954. doi: 10.1016/S0735-1097(02)02560-3. - DOI - PubMed
-
- Sabik JF, 3rd, Blackstone EH, Gillinov AM, et al. Occurrence and risk factors for reintervention after coronary artery bypass grafting. Circulation. 2006;114(1 Suppl):I454–I460. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
