

Imbalance of Th17, Treg, and helper innate lymphoid cell in the peripheral blood of patients with rheumatoid arthritis
- PMID: 35925523
- PMCID: PMC9652246
- DOI: 10.1007/s10067-022-06315-8
Imbalance of Th17, Treg, and helper innate lymphoid cell in the peripheral blood of patients with rheumatoid arthritis
Abstract
Introduction: Rheumatoid arthritis (RA) is a chronic inflammatory disease involving a variety of immune cells, including adaptive T and B cells and innate lymphoid cells (ILCs). Understanding the pathogenic role of these immune cells in RA provides new insights into the intervention and treatment of RA.
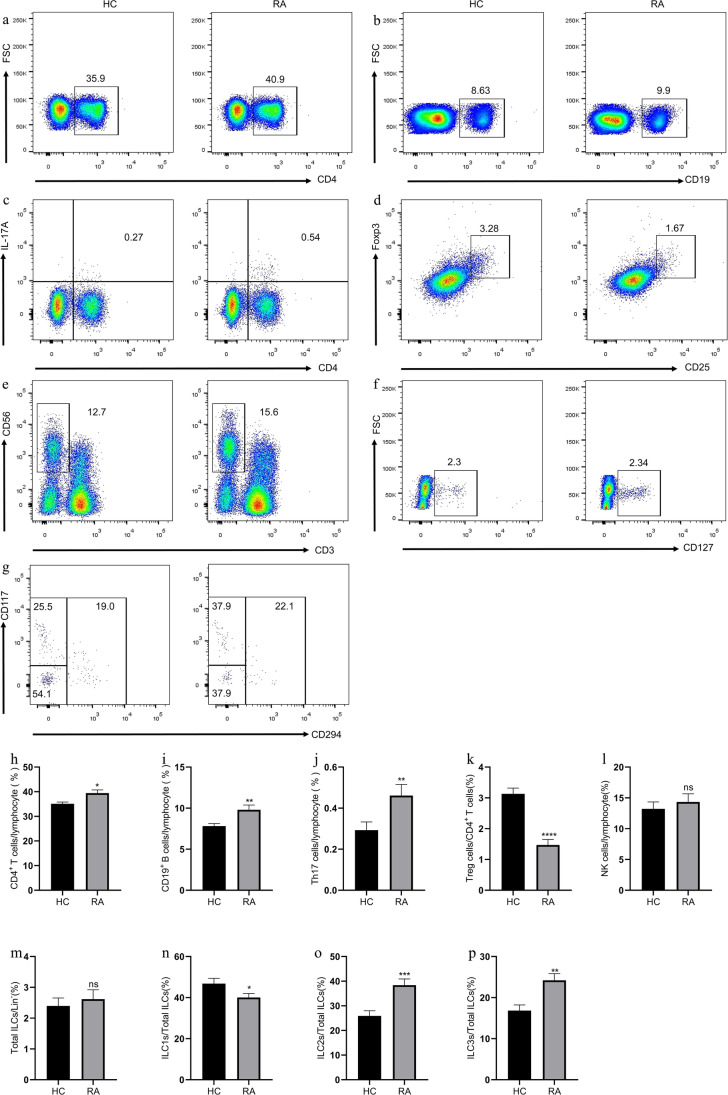
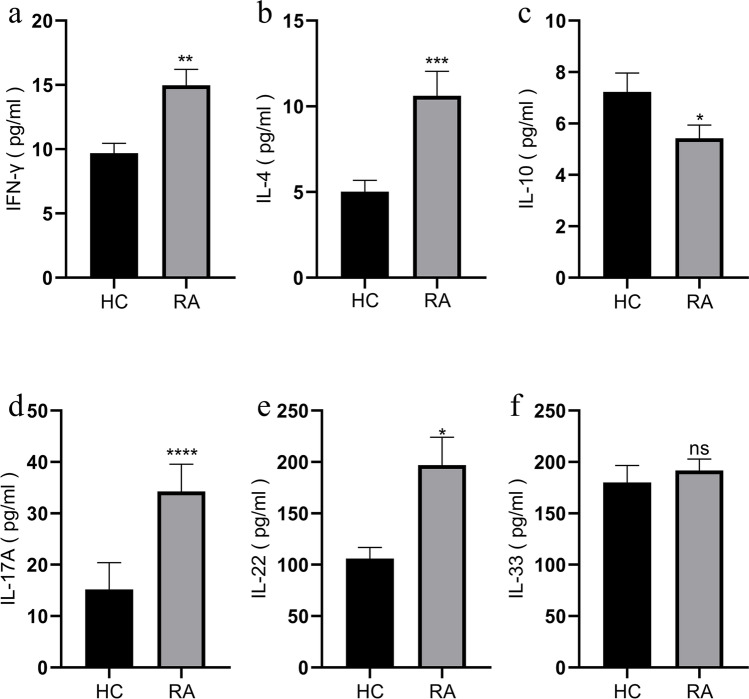
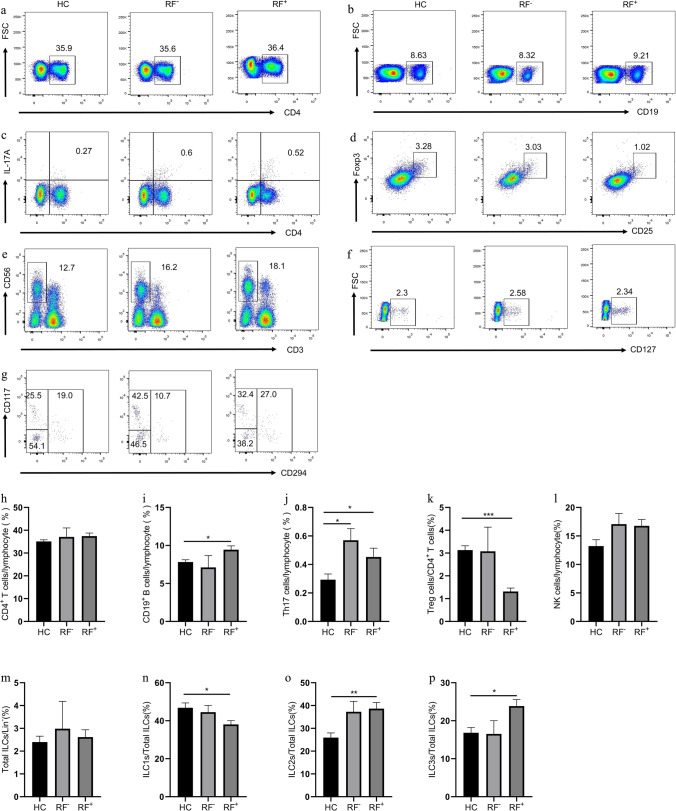
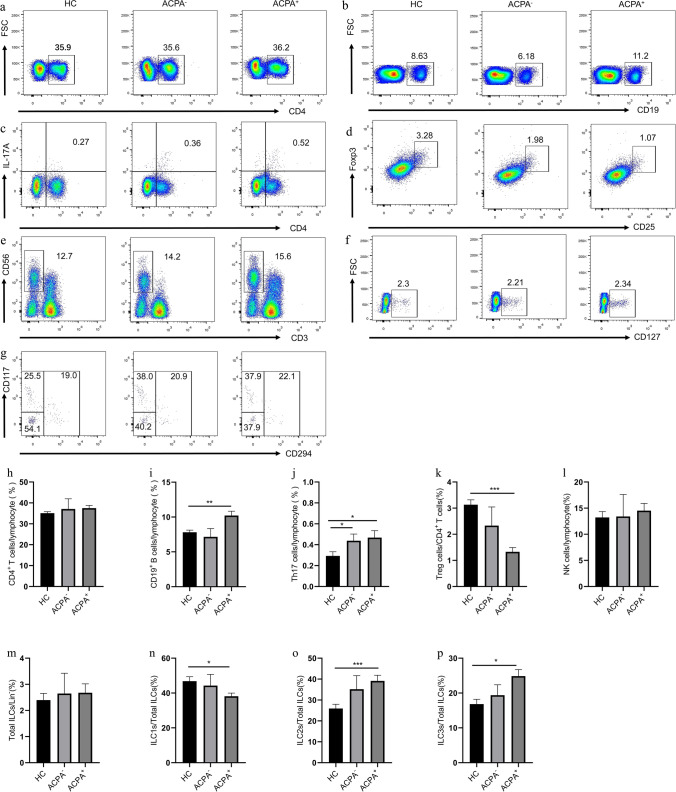
Methods: A total of 86 patients with RA (RA group) and 50 healthy controls (HC) were included in the study. The immune cells of CD4+, CD19+ B, NK, Th17, Treg, ILCs, and their subsets (i.e., ILC1s, ILC2s, and ILC3s) were characterized in peripheral blood mononuclear cells by flow cytometry. Cytokines (i.e., IFN-γ, IL-4, IL-10, IL-17A, IL-22, and IL-33) in sera were detected using ELISA. The above immune cells and cytokines were analyzed in patients with different disease activity status and positive ( +) or negative ( -) rheumatoid factor (RF)/anti-citrullinated protein antibodies (ACPA).
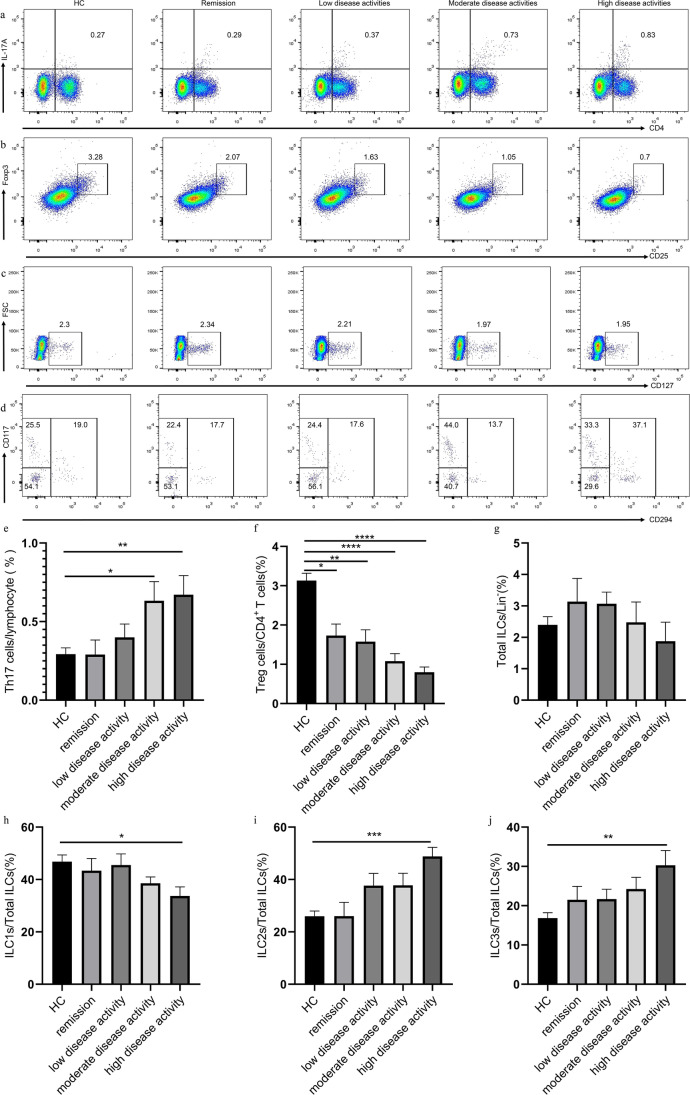
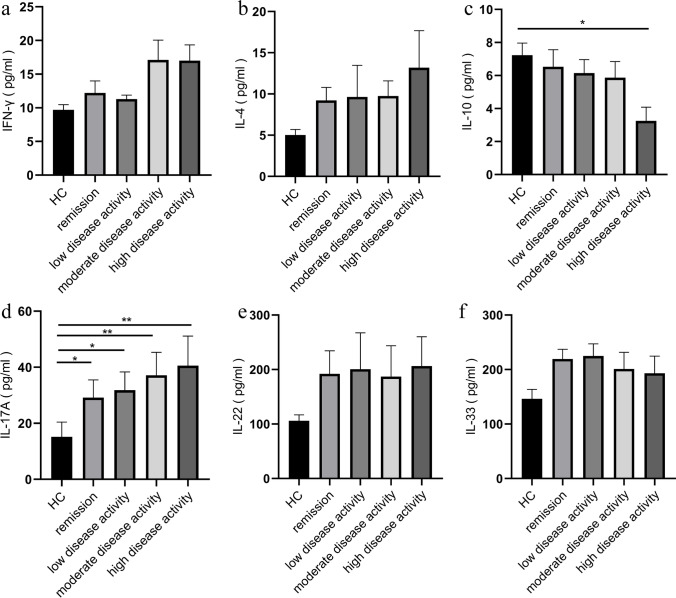
Results: Patients with RA had higher percentages of CD4+ T, CD19+ B, Th17, ILC2s, and ILC3s and lower percentages of Treg and ILC1s than HC. Patients with RA had elevated levels of IFN-γ, IL-4, IL-17A, and IL-22 and decreased level of IL-10. Compared with HC, patients with high disease activity had higher percentages of Th17, ILC2s, and ILC3s; lower percentages of ILC1s; and lower level of IL-10. The percentage of Treg cells in remission, low, moderate, and high disease activities decreased, whereas the level of IL-17A increased compared with HC. Furthermore, RF+ or ACPA+ patients exhibited elevated percentages of CD19+ B, ILC2s, and ILC3s and had decreased percentage of ILC1s and Treg cells than HC. The percentage of Th17 cells increased in RF-/ACPA- and RF+/ACPA+ patients. However, the above immune cells between RF or ACPA positive and negative patients were not significantly different.
Conclusion: Th17, Treg, and ILC subset dysregulations are present in patients with RA but may not be associated with conventionally defined seropositive RF and ACPA. Key Points • Th17, Treg, and ILC subset dysregulations are present in patients with RA but may reflect inflammation rather than specific diseases and stages. • No difference for the distribution of Th17, Treg, and ILC subsets between RF+ and RF- patients and between ACPA+ and ACPA- patients. The screening spectrum of RF and ACPA serology should be expanded to elucidate the role of immune cells in RA pathogenesis.
Keywords: Helper innate lymphoid cell; Rheumatoid arthritis; Th17; Treg.
© 2022. The Author(s).
Figures
Similar articles
-
Innate Lymphoid Cells and T Cells Contribute to the Interleukin-17A Signature Detected in the Synovial Fluid of Patients With Juvenile Idiopathic Arthritis.Arthritis Rheumatol. 2019 Mar;71(3):460-467. doi: 10.1002/art.40731. Epub 2019 Jan 28. Arthritis Rheumatol. 2019. PMID: 30350355 Free PMC article.
-
Group 3 innate lymphoid cells promotes Th17 cells differentiation in rheumatoid arthritis.Clin Exp Rheumatol. 2024 Nov;42(11):2183-2193. doi: 10.55563/clinexprheumatol/ktbiqc. Epub 2024 Jun 6. Clin Exp Rheumatol. 2024. PMID: 38855957
-
Dysregulation of Innate Lymphoid Cells in Patients with Active Rheumatoid Arthritis and Mice with Collagen-Induced Arthritis.Mediators Inflamm. 2021 Feb 20;2021:1915068. doi: 10.1155/2021/1915068. eCollection 2021. Mediators Inflamm. 2021. PMID: 33688303 Free PMC article.
-
CD4 T Helper Cell Subsets and Related Human Immunological Disorders.Int J Mol Sci. 2020 Oct 28;21(21):8011. doi: 10.3390/ijms21218011. Int J Mol Sci. 2020. PMID: 33126494 Free PMC article. Review.
-
The role of interleukin-6 signalling and its therapeutic blockage in skewing the T cell balance in rheumatoid arthritis.Clin Exp Immunol. 2017 Jul;189(1):12-20. doi: 10.1111/cei.12966. Epub 2017 Apr 20. Clin Exp Immunol. 2017. PMID: 28369786 Free PMC article. Review.
Cited by
-
Individualized diagnosis of rheumatoid arthritis: A rank-based qualitative T cell-related signature.PLoS One. 2025 Jun 26;20(6):e0326027. doi: 10.1371/journal.pone.0326027. eCollection 2025. PLoS One. 2025. PMID: 40569958 Free PMC article.
-
Serum tryptophan-kynurenine metabolites served as biomarkers of disease activity in rheumatoid arthritis and linked to immune imbalance.Arthritis Res Ther. 2025 Jul 5;27(1):136. doi: 10.1186/s13075-025-03596-7. Arthritis Res Ther. 2025. PMID: 40618074 Free PMC article.
-
Circulating PCSK9 relates to aggravated disease activity, Th17/Treg imbalance, and predicts treatment outcome of conventional synthetic DMARDs in rheumatoid arthritis patients.Ir J Med Sci. 2023 Dec;192(6):3187-3194. doi: 10.1007/s11845-023-03323-8. Epub 2023 Feb 24. Ir J Med Sci. 2023. PMID: 36826711
-
Aberrant Subsets of Regulatory T Cells and their Correlations with Serum IL-2 in Patients with Rheumatoid Arthritis.Inflammation. 2025 Feb 19. doi: 10.1007/s10753-025-02248-x. Online ahead of print. Inflammation. 2025. PMID: 39971881
-
Influence of a Th17-Inducing Cytokine Milieu on Phenotypical and Functional Properties of Regulatory T Cells in Chronic Inflammatory Arthritis.Int J Mol Sci. 2025 Jul 29;26(15):7339. doi: 10.3390/ijms26157339. Int J Mol Sci. 2025. PMID: 40806470 Free PMC article.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
