

Use of Intraoperative Frozen Section to Assess Final Tumor Margin Status in Patients Undergoing Surgery for Oral Cavity Squamous Cell Carcinoma
- PMID: 35925571
- PMCID: PMC9353701
- DOI: 10.1001/jamaoto.2022.2131
Use of Intraoperative Frozen Section to Assess Final Tumor Margin Status in Patients Undergoing Surgery for Oral Cavity Squamous Cell Carcinoma
Abstract
Importance: Methods of assessing final margin status in patients undergoing surgery for oral cavity squamous cell carcinoma, such as intraoperative frozen section histopathology (IFSH) taken from the tumor bed, may have limitations in accuracy.
Objective: To evaluate the accuracy and implications of using IFSH samples to assess tumor bed margins in patients undergoing surgery for oral cavity squamous cell carcinoma (SCC).
Design, setting, and participants: This cross-sectional study included 1257 patients who underwent surgery for oral cavity SCC between January 1, 2000, and December 31, 2015, at an academic cancer center. A total of 4821 IFSH samples were examined from 1104 patients (87.8%) who had at least 1 IFSH sample. Institutional practice is to harvest margins for IFSH from the tumor bed. Statistical analysis was performed from August 1, 2021, to April 4, 2022.
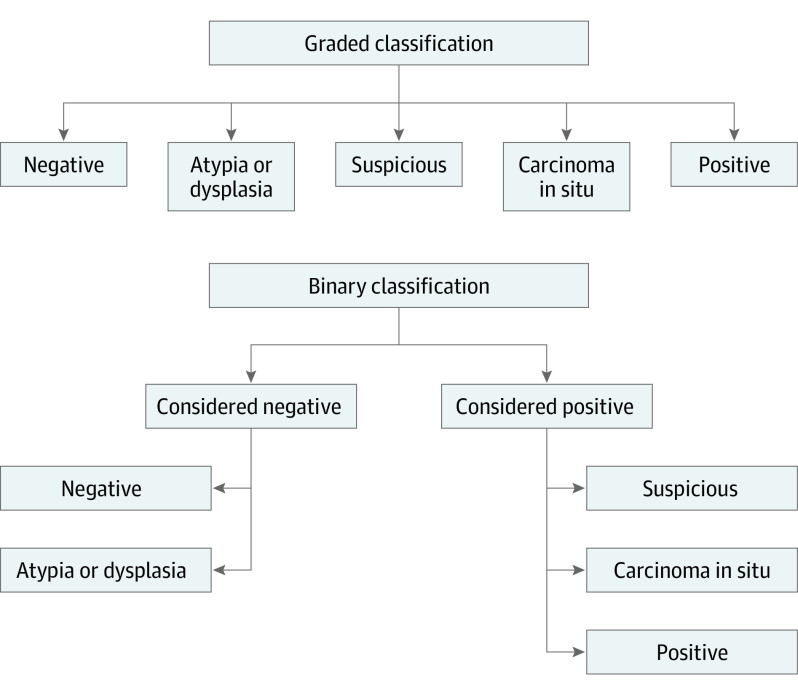
Main outcomes and measures: Sensitivity and specificity were calculated for IFSH samples of margins compared with the permanent pathology samples of the same tissue and for IFSH compared with the final tumor specimen histopathology (FTSH). Results were classified using a binary method, with histopathologic reports interpreted as either negative (including negative or atypia or dysplasia) or positive (including carcinoma in situ, suspicious, or positive).
Results: A total of 1257 patients met the inclusion criteria, including 709 men (56.4%), with a median age of 62 years (IQR, 52-73 years); 1104 patients (627 men [56.8%]; median age, 62 years [IQR, 52-72 years]) had IFHS samples. For IFSH relative to permanent sections of the IFSH tissue, sensitivity and specificity of IFSH were high (sensitivity, 76.5% [95% CI, 67.5%-85.5%]; specificity, 99.9% [95% CI, 99.8%-100%]), with discordant results in 24 of 4821 total specimens (0.5%). Final specimen margins were positive in 11.7% of patients (147 of 1257). Compared with FTSH, the sensitivity of IFSH for defining margin status was 10.8% (95% CI, 5.8%-15.8%), and the specificity was 99.1% (95% CI, 98.8%-99.4%). The rate of discordance was 4.0% (171 of 4284 specimens) between IFSH and FTSH.
Conclusions and relevance: The findings of this cross-sectional study suggest that IFSH is accurate compared with permanent pathologic characteristics of the same tissue, but less reliable at assessing final margin status on the tumor specimen. Despite a high specificity, the sensitivity of IFSH compared with FTSH is low, which may be associated with the inherent inability of tumor bed IFSH margin analysis to accurately account for the 3-dimensional association of tumor margins with the periphery of the specimen and the overall low rate of positive final tumor margins. Although tumor bed IFSH is widely used in the management of oral cavity cancer, this study suggests that there are limitations of this modality in assessing the final surgical margin status.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
