

Predictors beyond the lesion: Health and demographic factors associated with aphasia severity
- PMID: 35926368
- PMCID: PMC11205278
- DOI: 10.1016/j.cortex.2022.06.013
Predictors beyond the lesion: Health and demographic factors associated with aphasia severity
Abstract
Background: Lesion-related factors are associated with severity of language impairment in persons with aphasia. The extent to which demographic and health factors predict language impairment beyond traditional cortical measures remains unknown. Identifying and understanding the contributions of factors to predictive models of severity constitutes critical knowledge for clinicians interested in charting the likely course of aphasia in their patients and designing effective treatment approaches in light of those predictions.
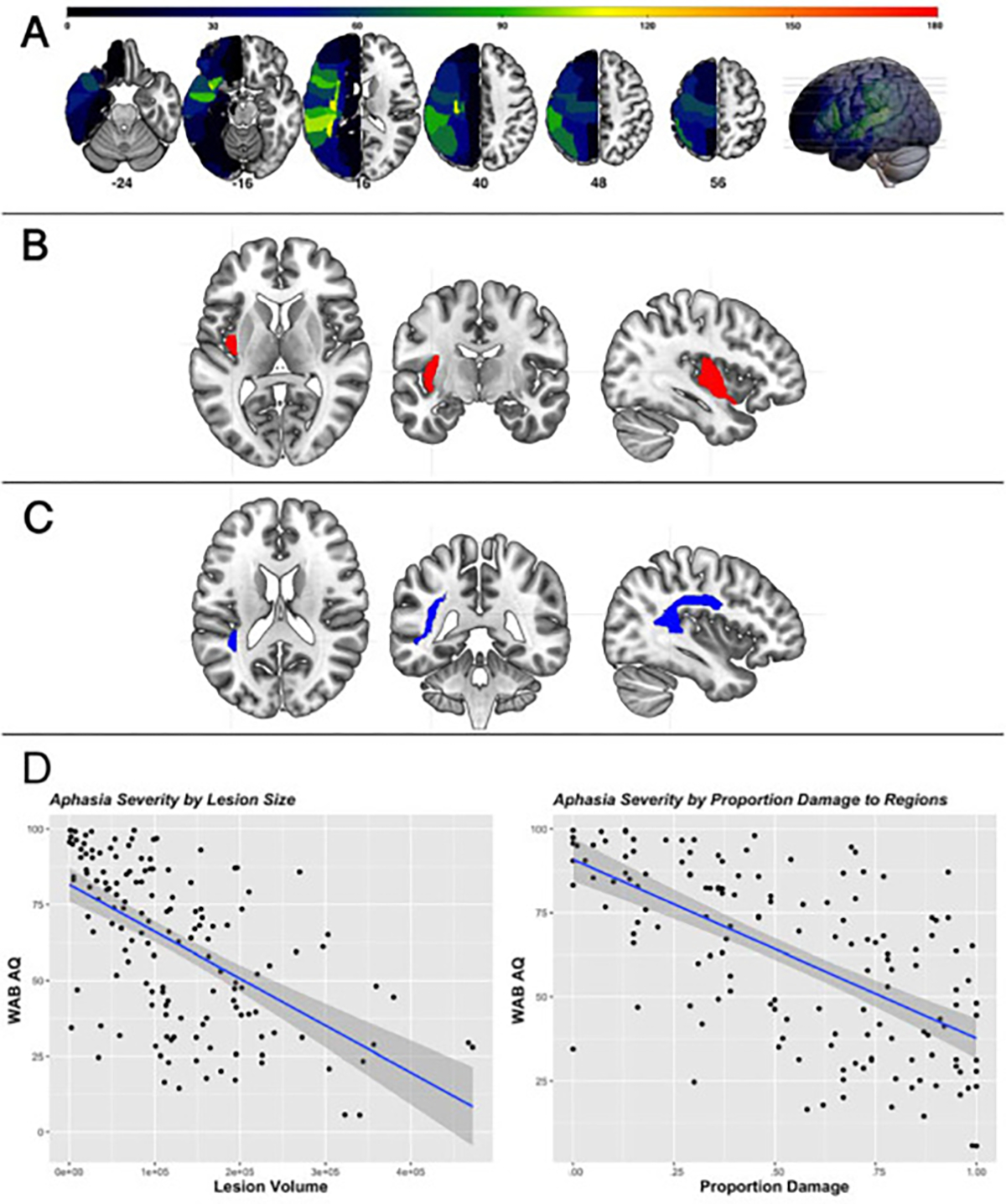
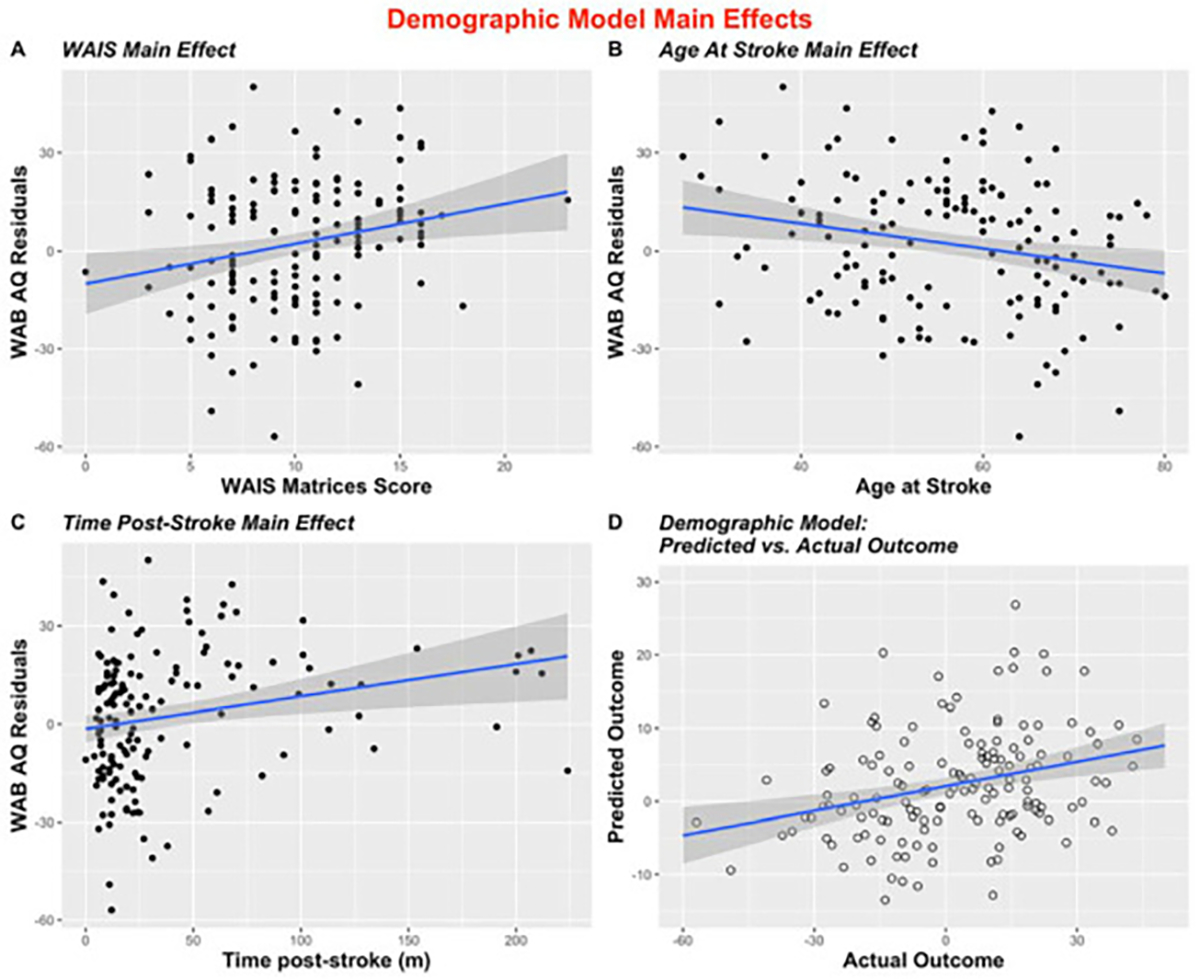
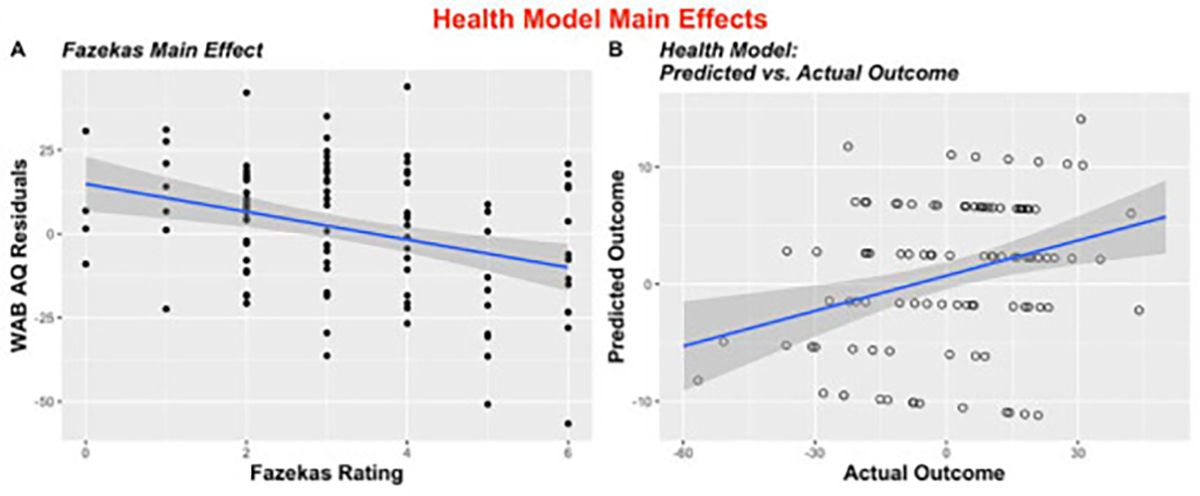
Methods: Utilizing neuroimaging and language testing from our cohort of 224 individuals in the chronic stage of recovery from a left-hemisphere stroke in a cross-sectional study, we first conducted a lesion symptom mapping (LSM) analysis to identify regions associated with aphasia severity scores. After controlling for lesion volume and damage to pre-identified areas, three models were created to predict severity scores: 1) Demographic Model (N = 147); 2) Health Model (N = 106); and 3) Overall Model (N = 106). Finally, all identified factors were entered into a Final Model to predict raw severity scores.
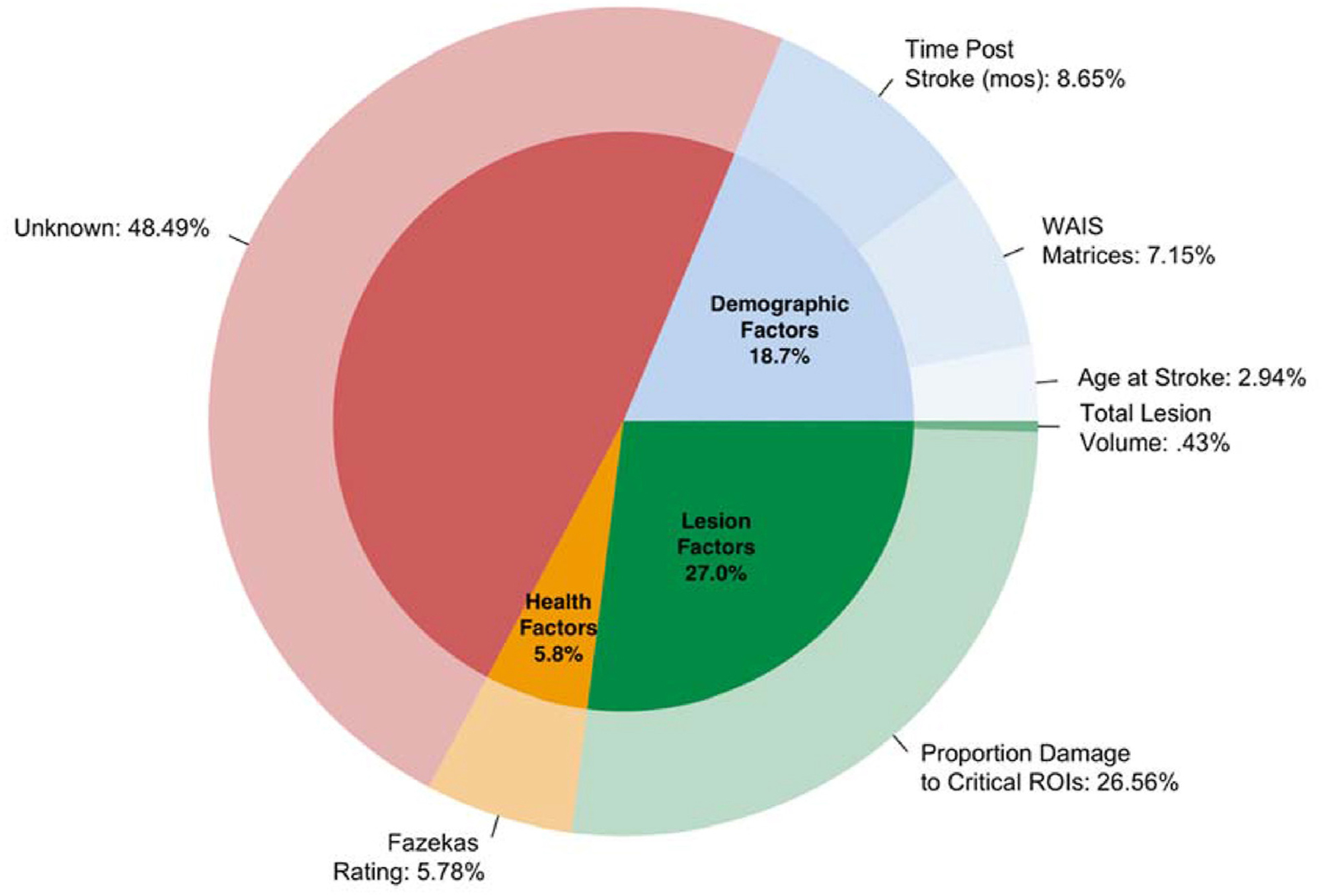
Results: Two areas were associated with aphasia severity-left posterior insula and left arcuate fasciculus. The results from the Demographic Model revealed non-linguistic cognitive ability, age at stroke, and time post-stroke as significant predictors of severity (P = .005; P = .02; P = .001, respectively), and results from the Health Model suggested the extent of leukoaraiosis is associated with severity (P = .0004). The Overall Model showed a relationship between aphasia severity and cognitive ability (P = .01), time post-stroke (P = .002), and leukoaraiosis (P = .01). In the Final Model, which aimed to predict raw severity scores, demographic, health, and lesion factors explained 55% of the variance in severity, with health and demographic factors uniquely explaining nearly half of performance variance.
Conclusions: Results from this study add to the literature suggesting patient-specific variables can shed light on individual differences in severity beyond lesion factors. Additionally, our results emphasize the importance of non-linguistic cognitive ability and brain health in aphasia recovery.
Keywords: Aging; Aphasia; Leukoaraiosis; Recovery; Stroke.
Copyright © 2022. Published by Elsevier Ltd.
Figures
Similar articles
-
Leukoaraiosis Is Associated With a Decline in Language Abilities in Chronic Aphasia.Neurorehabil Neural Repair. 2019 Sep;33(9):718-729. doi: 10.1177/1545968319862561. Epub 2019 Jul 17. Neurorehabil Neural Repair. 2019. PMID: 31315507 Free PMC article.
-
Leukoaraiosis is independently associated with naming outcome in poststroke aphasia.Neurology. 2018 Aug 7;91(6):e526-e532. doi: 10.1212/WNL.0000000000005945. Epub 2018 Jul 6. Neurology. 2018. PMID: 29980639 Free PMC article.
-
Anatomical predictors of aphasia recovery: a tractography study of bilateral perisylvian language networks.Brain. 2014 Jul;137(Pt 7):2027-39. doi: 10.1093/brain/awu113. Brain. 2014. PMID: 24951631
-
Post-stroke aphasia prognosis: a review of patient-related and stroke-related factors.J Eval Clin Pract. 2012 Jun;18(3):689-94. doi: 10.1111/j.1365-2753.2011.01650.x. Epub 2011 Mar 13. J Eval Clin Pract. 2012. PMID: 21395923 Review.
-
Factors predicting post-stroke aphasia recovery.J Neurol Sci. 2015 May 15;352(1-2):12-8. doi: 10.1016/j.jns.2015.03.020. Epub 2015 Mar 20. J Neurol Sci. 2015. PMID: 25888529 Review.
Cited by
-
Dissociating reading and auditory comprehension in persons with aphasia.Brain Commun. 2024 Mar 25;6(2):fcae102. doi: 10.1093/braincomms/fcae102. eCollection 2024. Brain Commun. 2024. PMID: 38585671 Free PMC article.
-
Early subacute frontal callosal microstructure and language outcomes after stroke.Brain Commun. 2025 Jan 21;7(1):fcae370. doi: 10.1093/braincomms/fcae370. eCollection 2025. Brain Commun. 2025. PMID: 39845737 Free PMC article.
-
Long-range white matter fibres and post-stroke verbal and non-verbal cognition.Brain Commun. 2024 Aug 16;6(4):fcae262. doi: 10.1093/braincomms/fcae262. eCollection 2024. Brain Commun. 2024. PMID: 39185028 Free PMC article.
-
Under pressure: the interplay of hypertension and white matter hyperintensities with cognition in chronic stroke aphasia.Brain Commun. 2024 Jun 11;6(3):fcae200. doi: 10.1093/braincomms/fcae200. eCollection 2024. Brain Commun. 2024. PMID: 38894950 Free PMC article.
-
Predicting Language Function Post-Stroke: A Model-Based Structural Connectivity Approach.Neurorehabil Neural Repair. 2024 Jun;38(6):447-459. doi: 10.1177/15459683241245410. Epub 2024 Apr 11. Neurorehabil Neural Repair. 2024. PMID: 38602161 Free PMC article.
References
-
- Baldo J, Bunge S, Wilson SM, & Dronkers NF (2010). Is relational reasoning dependent on language? A voxel- based lesion symptom mapping study. Brain and Language, 113(2), 59–64. 10.1016/j.bandl.2010.01.004.Is - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
