

Efficacy and Safety of the Safe Triangular Working Zone Approach in Percutaneous Vertebroplasty for Spinal Metastasis
- PMID: 35926840
- PMCID: PMC9434739
- DOI: 10.3348/kjr.2021.0914
Efficacy and Safety of the Safe Triangular Working Zone Approach in Percutaneous Vertebroplasty for Spinal Metastasis
Abstract
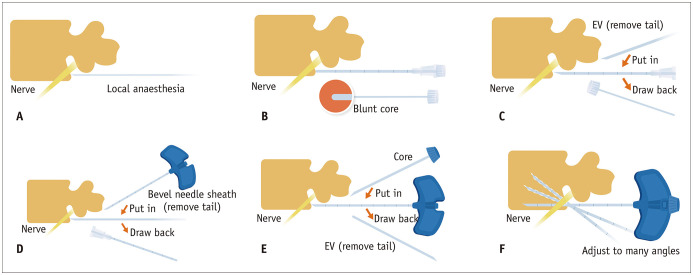
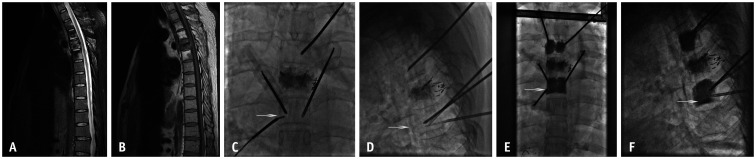
Objective: This study aimed to assess the technical feasibility, efficacy, and safety of the safe triangular working zone (STWZ) approach applied in percutaneous vertebroplasty (PV) for spinal metastases involving the posterior part of the vertebral body.
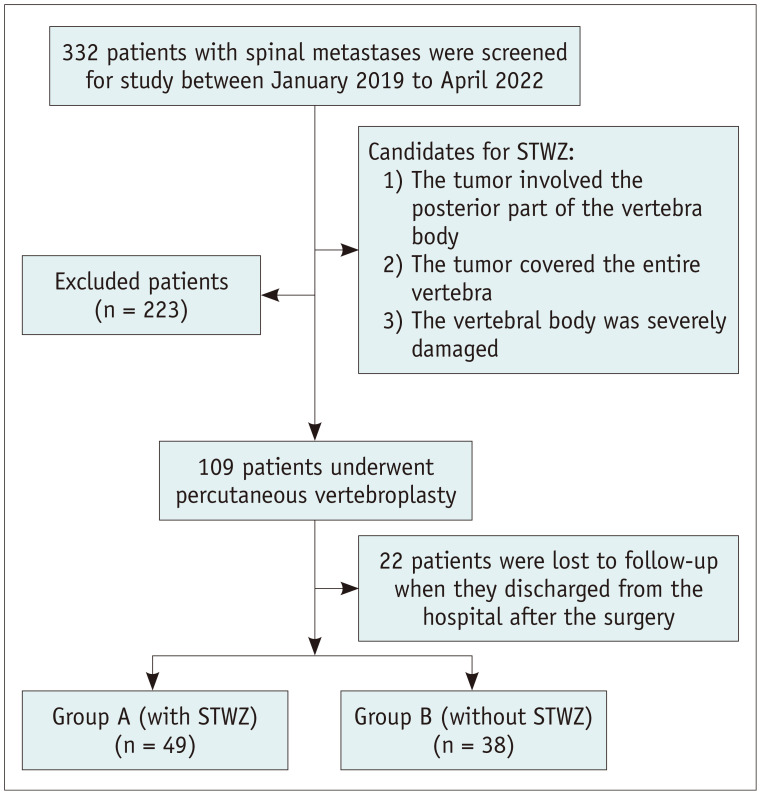
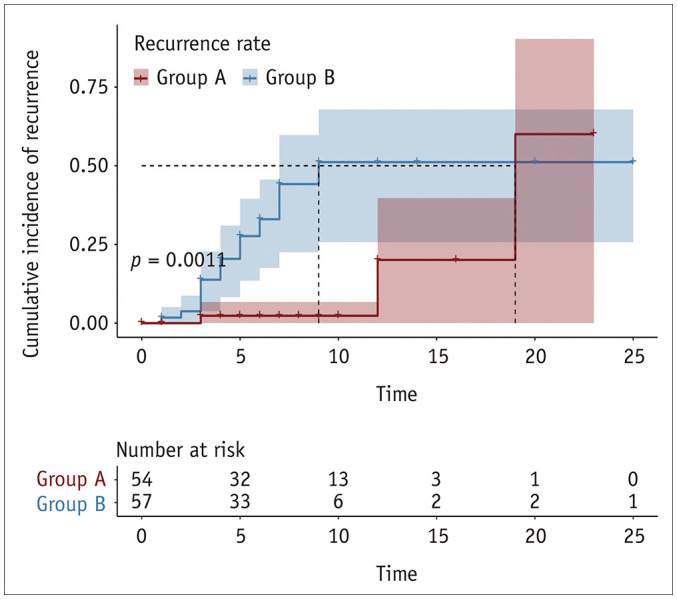
Materials and methods: We prospectively enrolled 87 patients who underwent PV for spinal metastasis involving the posterior part of the vertebral body, with or without the STWZ approach, from January 2019 to April 2022. Forty-nine patients (27 females and 22 males; mean age ± standard deviation [SD], 57.2 ± 11.6 years; age range, 31-76 years) were included in group A (with STWZ approach), accounting for 54 vertebrae. Thirty-eight patients (18 females and 20 males; 59.1 ± 10.9 years; 29-81 years) were included in group B (without STWZ approach), accounting for 57 vertebrae. Patient demographics, procedure-related variables, and pain relief as assessed using the visual analog scale (VAS) were collected at different time points. Tumor recurrence in the vertebrae after PV was analyzed using Kaplan-Meier curves.
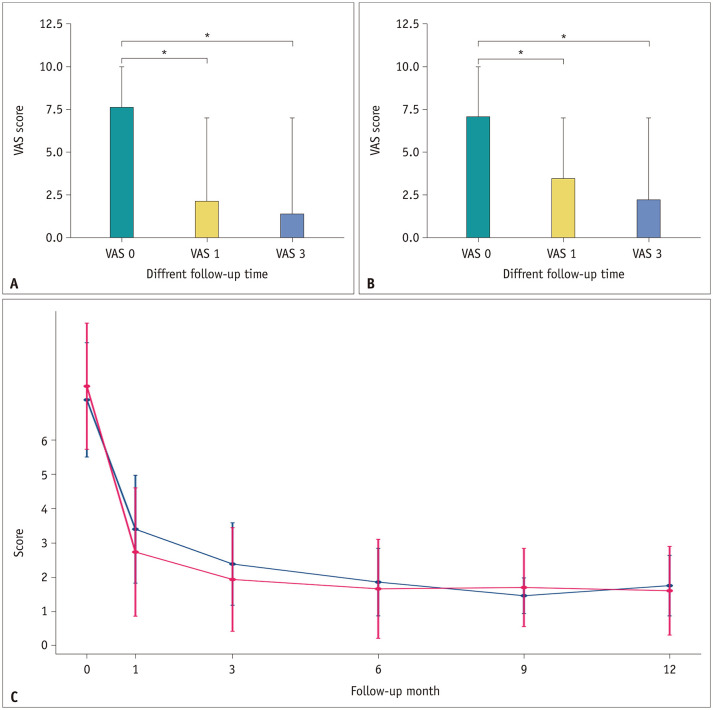
Results: The STWZ approach was successful from T1 to L5 without severe complications. Cement filling was satisfactory in 47/54 (87.0%) and 25/57 (43.9%) vertebrae in groups A and B, respectively (p < 0.001). Cement leakage was not significantly different between groups A and B (p = 1.000). Mean VAS score ± SD before and 1 week and 1, 3, 6, 9, and 12 months after PV were 7.6 ± 1.8, 4.2 ± 2.0, 2.7 ± 1.9, 1.9 ± 1.5, 1.7 ± 1.4, 1.7 ± 1.1, and 1.6 ± 1.3, respectively, in group A and 7.2 ± 1.7, 4.0 ± 1.3, 3.4 ± 1.6, 2.4 ± 1.2, 1.8 ± 1.0, 1.4 ± 0.5, and 1.7 ± 0.9, respectively, in group B. Kaplan-Meier analysis showed a lower tumor recurrence rate in group A than in group B (p = 0.001).
Conclusion: The STWZ approach may represent a new, safe, alternative/auxiliary approach to target the posterior part of the vertebral body in the PV for spinal metastases.
Keywords: Percutaneous vertebroplasty; Puncture approach; Spinal metastases.
Copyright © 2022 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Tsoumakidou G, Too CW, Koch G, Caudrelier J, Cazzato RL, Garnon J, et al. CIRSE guidelines on percutaneous vertebral augmentation. Cardiovasc Intervent Radiol. 2017;40:331–342. - PubMed
-
- Ringer AJ, Bhamidipaty SV. Percutaneous access to the vertebral bodies: a video and fluoroscopic overview of access techniques for trans-, extra-, and infrapedicular approaches. World Neurosurg. 2013;80:428–435. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
