

Coronary Atherosclerosis, Cardiac Troponin, and Interleukin-6 in Patients With Chest Pain: The PROMISE Trial Results
- PMID: 35926901
- PMCID: PMC9353061
- DOI: 10.1016/j.jcmg.2022.03.016
Coronary Atherosclerosis, Cardiac Troponin, and Interleukin-6 in Patients With Chest Pain: The PROMISE Trial Results
Abstract
Background: Increased inflammation and myocardial injury can be observed in the absence of myocardial infarction or obstructive coronary artery disease (CAD).
Objectives: The authors determined whether biomarkers of inflammation and myocardial injury-interleukin (IL)-6 and high-sensitivity cardiac troponin (hs-cTn)-were associated with the presence and extent of CAD and were independent predictors of major adverse cardiovascular events (MACEs) in stable chest pain.
Methods: Using participants from the PROMISE trial, the authors measured hs-cTn I and IL-6 concentrations and analyzed computed tomography angiography (CTA) images in the core laboratory for CAD characteristics: significant stenosis (≥70%), high-risk plaque (HRP), Coronary Artery Disease Reporting and Data System (CAD-RADS) categories, segment involvement score (SIS), and coronary artery calcium (CAC) score. The primary endpoint was a composite MACE (death, myocardial infarction, or unstable angina).
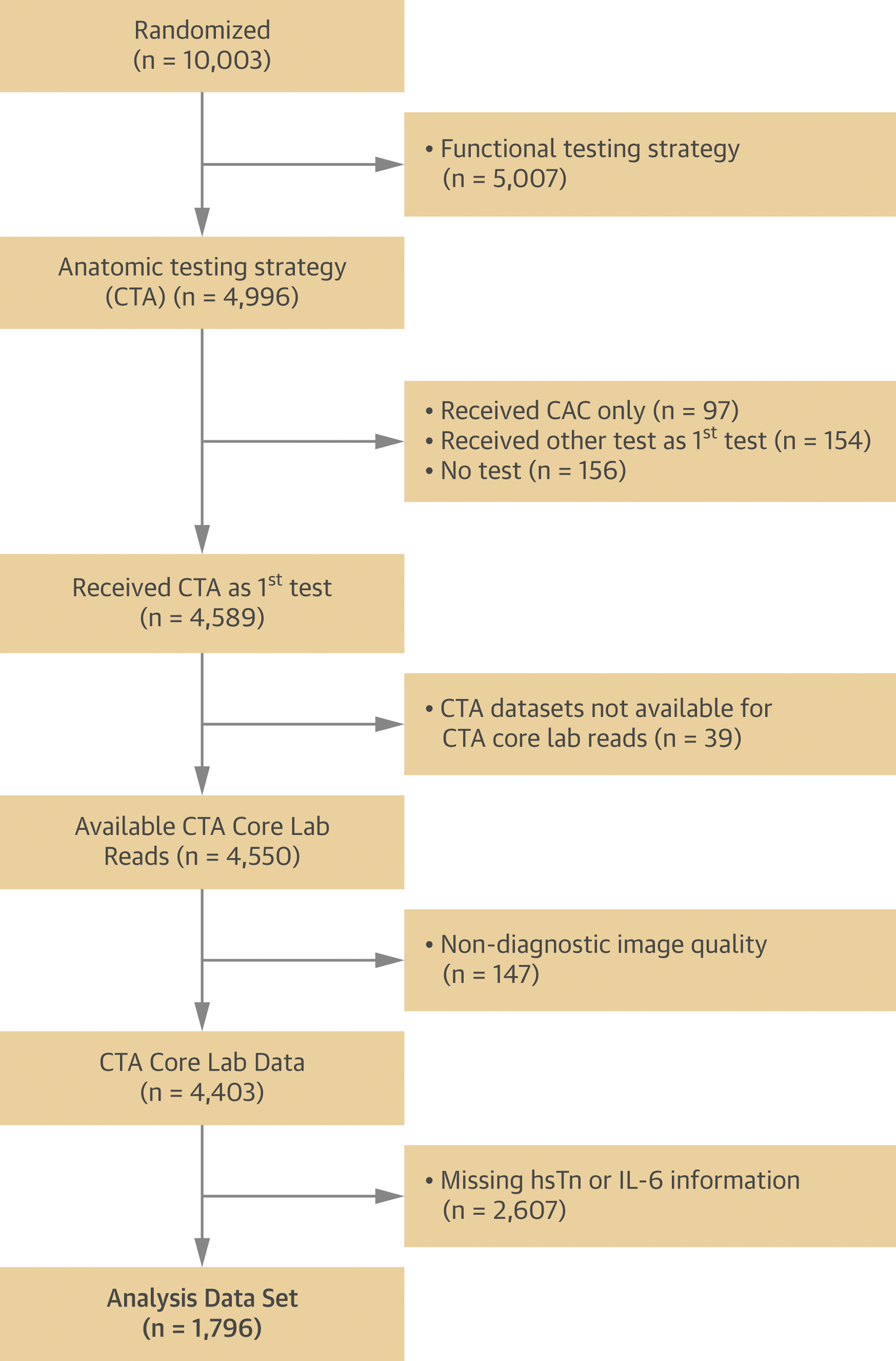
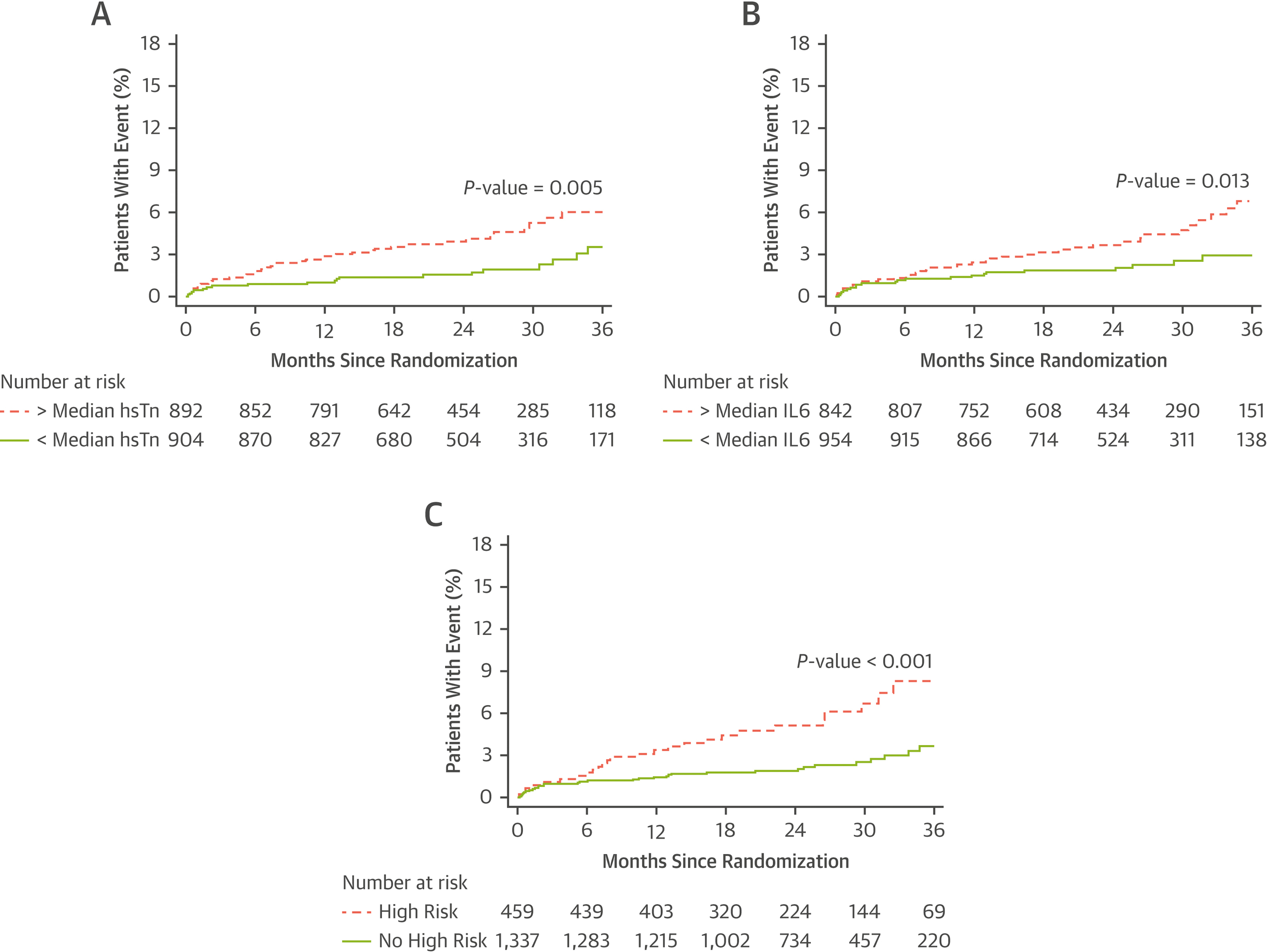
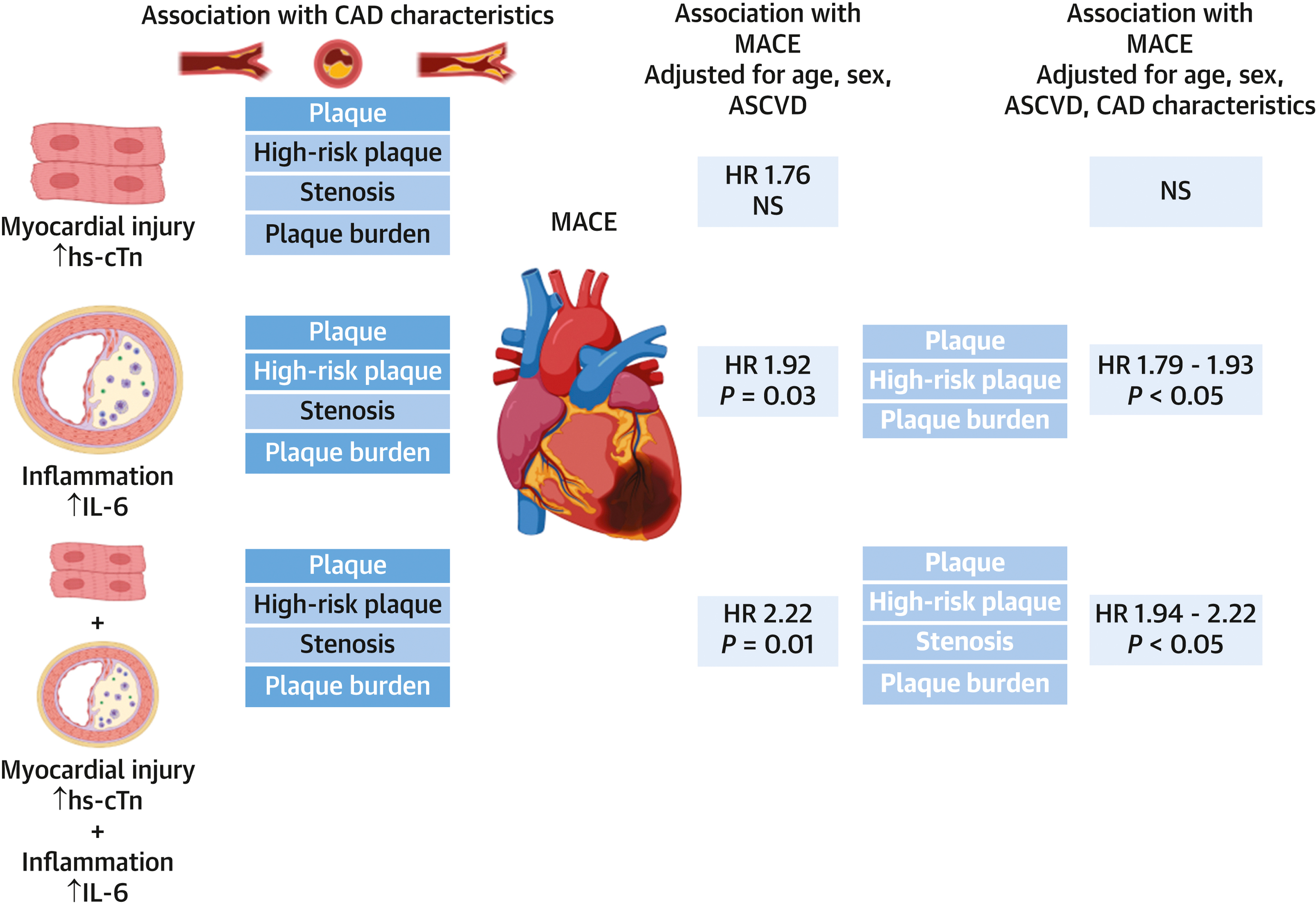
Results: The authors included 1,796 participants (age 60.2 ± 8.0 years; 47.5% men, median follow-up 25 months). In multivariable linear regression adjusted for atherosclerotic cardiovascular disease (ASCVD) risk, hs-cTn was associated with HRP, stenosis, CAD-RADS, and SIS. IL-6 was only associated with stenosis and CAD-RADS. hs-cTn above median (1.5 ng/L) was associated with MACEs in univariable analysis (HR: 2.1 [95% CI: 1.3-3.6]; P = 0.006), but not in multivariable analysis adjusted for ASCVD and CAD. IL-6 above median (1.8 ng/L) was associated with MACEs in multivariable analysis adjusted for ASCVD and HRP (HR: 1.9 [95% CI: 1.1-3.3]; P = 0.03), CAC (HR: 1.9 [95% CI: 1.0-3.4]; P = 0.04), and SIS (HR: 1.8 [95% CI: 1.0-3.2]; P = 0.04), but not for stenosis or CAD-RADS. In participants with nonobstructive CAD (stenosis 1%-69%), the presence of both hs-cTn and IL-6 above median was strongly associated with MACEs (HR: 2.5-2.7 after adjustment for CAD characteristics).
Conclusions: Concentrations of hs-cTn and IL-6 were associated with CAD characteristics and MACEs, indicating that myocardial injury and inflammation may each contribute to pathways in CAD pathophysiology. This association was most pronounced among participants with nonobstructive CAD representing an opportunity to tailor treatment in this at-risk group. (PROspective Multicenter Imaging Study for Evaluation of Chest Pain [PROMISE]; NCT01174550).
Keywords: biomarkers; computed tomography angiography; coronary atherosclerotic plaque; high-sensitivity cardiac troponin; interleukin 6.
Copyright © 2022 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The PROMISE trial was funded by grants R01HL098237, R01HL098236, R01HL98305, and R01HL098235 from the National Heart, Lung, and Blood Institute (NHLBI). The funding source had no role in the design and conduct of this study, study analyses and interpretation of the data, the drafting and editing of the manuscript and its final contents, approval of the manuscript, and the decision to submit the manuscript for publication. The views expressed in this article do not necessarily represent the official views of the NHLBI. This article was prepared while Dr Ginsburg was employed at Duke University. The opinions expressed in this article are the author’s own and do not reflect the view of the National Institutes of Health, the Department of Health and Human Services, or the United States government. Dr Ferencik has received a grant from the American Heart Association, National Institutes of Health; and has received consulting fees from Biograph, Inc. Dr Bittner was supported by a grant from the National Institutes of Health/NHLBI (5K24HL113128). Dr Lu has received grant support from the American Roentgen Ray Society Scholarship during the conduct of the study; and has received personal fees from PQBypass outside of the submitted work. Dr Meyersohn was supported by National Institutes of Health/NHLBI (T32 HL076136). Dr Douglas has received grant support from HeartFlow; and has served on a data and safety monitoring board for GE HealthCare outside of the submitted work. Dr Hoffmann has received grants from the American College of Radiology Imaging Network and HeartFlow during the conduct of the study, and from Siemens Healthcare outside of the submitted work. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Potential Markers of Coronary Artery Plaque and Future Events: Are They Right Under Our Nose?JACC Cardiovasc Imaging. 2022 Aug;15(8):1439-1441. doi: 10.1016/j.jcmg.2022.05.013. JACC Cardiovasc Imaging. 2022. PMID: 35926902 No abstract available.
References
-
- Williams MC, Kwiecinski J, Doris M, et al. Low-Attenuation Noncalcified Plaque on Coronary Computed Tomography Angiography Predicts Myocardial Infarction: Results From the Multicenter SCOT-HEART Trial (Scottish Computed Tomography of the HEART). Circulation 2020;141(18):1452–62. Doi: 10.1161/CIRCULATIONAHA.119.044720. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
