

Molecular characterization of colorectal cancer related peritoneal metastatic disease
- PMID: 35927254
- PMCID: PMC9352687
- DOI: 10.1038/s41467-022-32198-z
Molecular characterization of colorectal cancer related peritoneal metastatic disease
Abstract
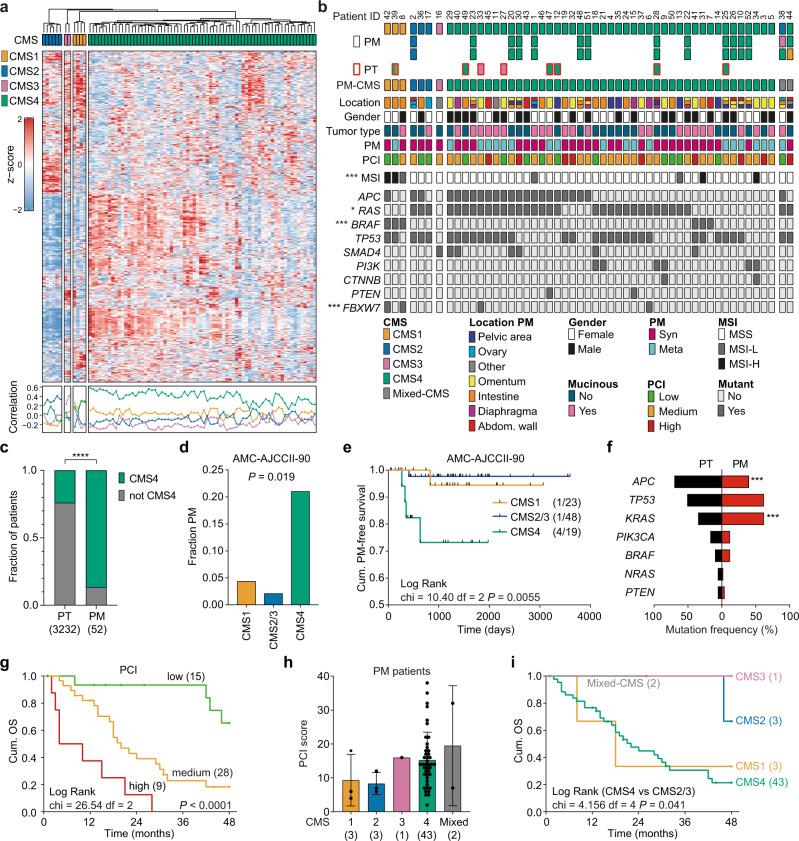
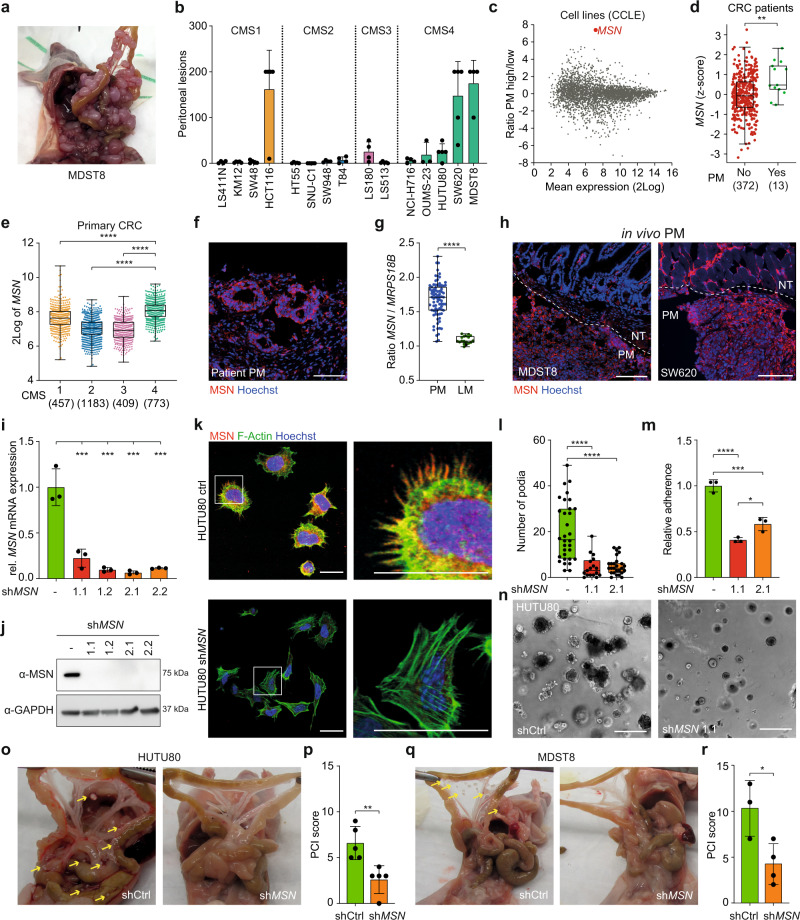
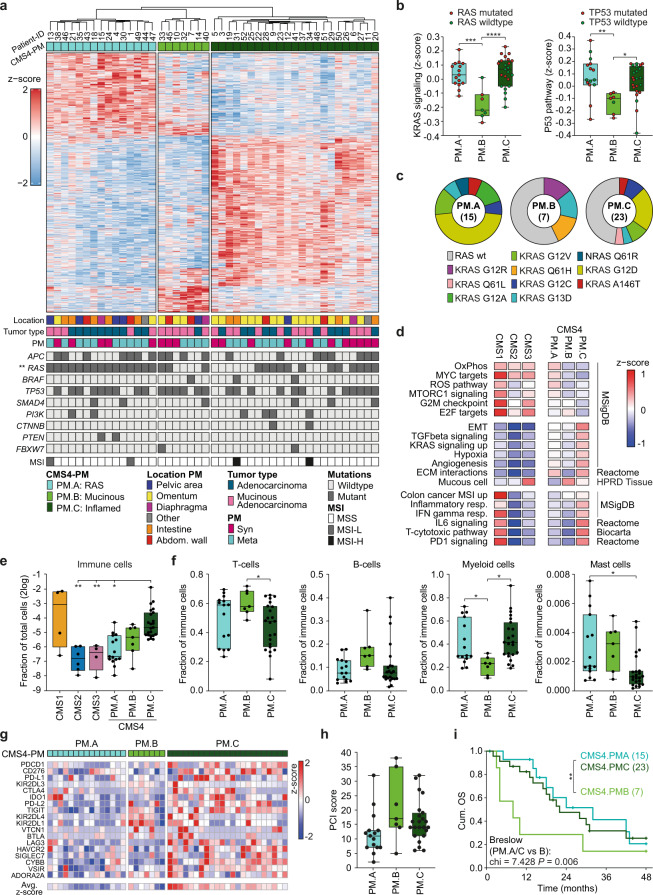
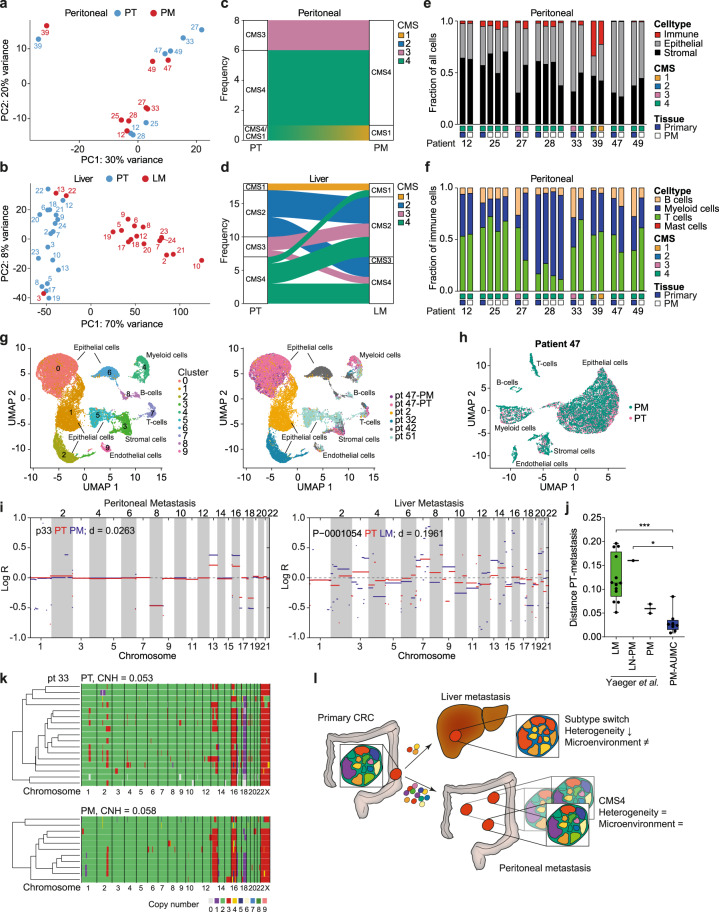
A significant proportion of colorectal cancer (CRC) patients develop peritoneal metastases (PM) in the course of their disease. PMs are associated with a poor quality of life, significant morbidity and dismal disease outcome. To improve care for this patient group, a better understanding of the molecular characteristics of CRC-PM is required. Here we present a comprehensive molecular characterization of a cohort of 52 patients. This reveals that CRC-PM represent a distinct CRC molecular subtype, CMS4, but can be further divided in three separate categories, each presenting with unique features. We uncover that the CMS4-associated structural protein Moesin plays a key role in peritoneal dissemination. Finally, we define specific evolutionary features of CRC-PM which indicate that polyclonal metastatic seeding underlies these lesions. Together our results suggest that CRC-PM should be perceived as a distinct disease entity.
© 2022. The Author(s).
Conflict of interest statement
L.V. received consultancy fees from Bayer, MSD, Genentech, Servier and Pierre Fabre, but these had no relation to the content of this publication. I.H.d.H. received research funding (paid to institute) from Roche and RandD for unrelated research. R.K., F.P.D., N.S., and G.A.S. are employees of and have ownership interest in Celsius Therapeutics. All other authors declare no conflict of interest in the context of this publication.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
