

Homotypic and heterotypic immune responses to Omicron variant in immunocompromised patients in diverse clinical settings
- PMID: 35927279
- PMCID: PMC9352686
- DOI: 10.1038/s41467-022-32235-x
Homotypic and heterotypic immune responses to Omicron variant in immunocompromised patients in diverse clinical settings
Abstract
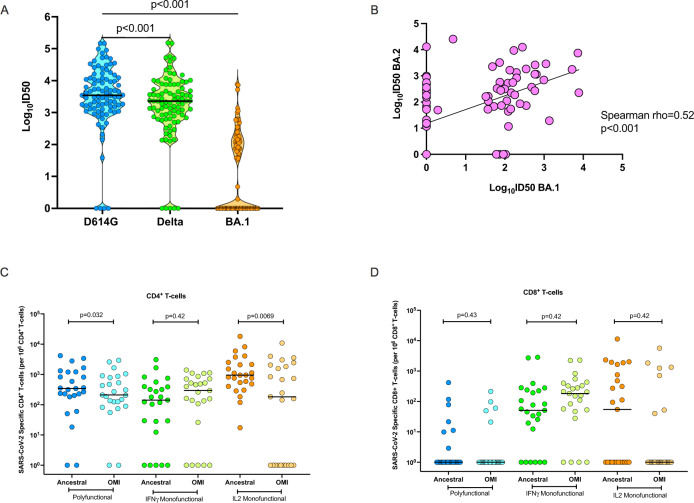
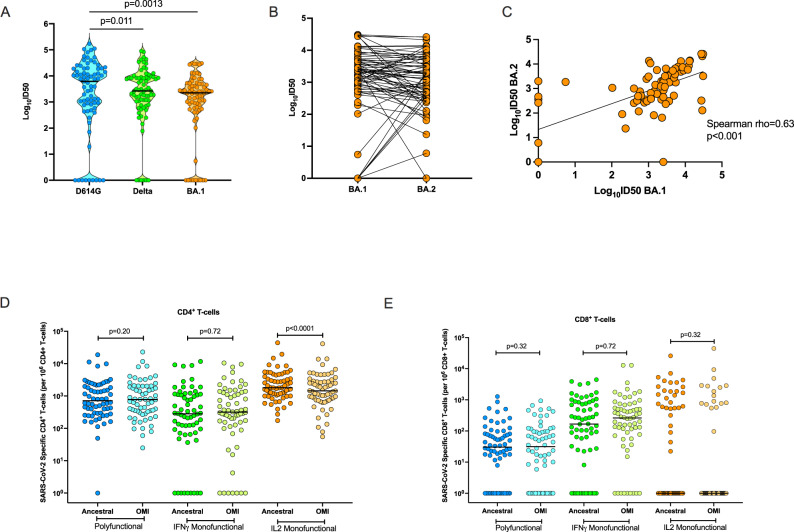
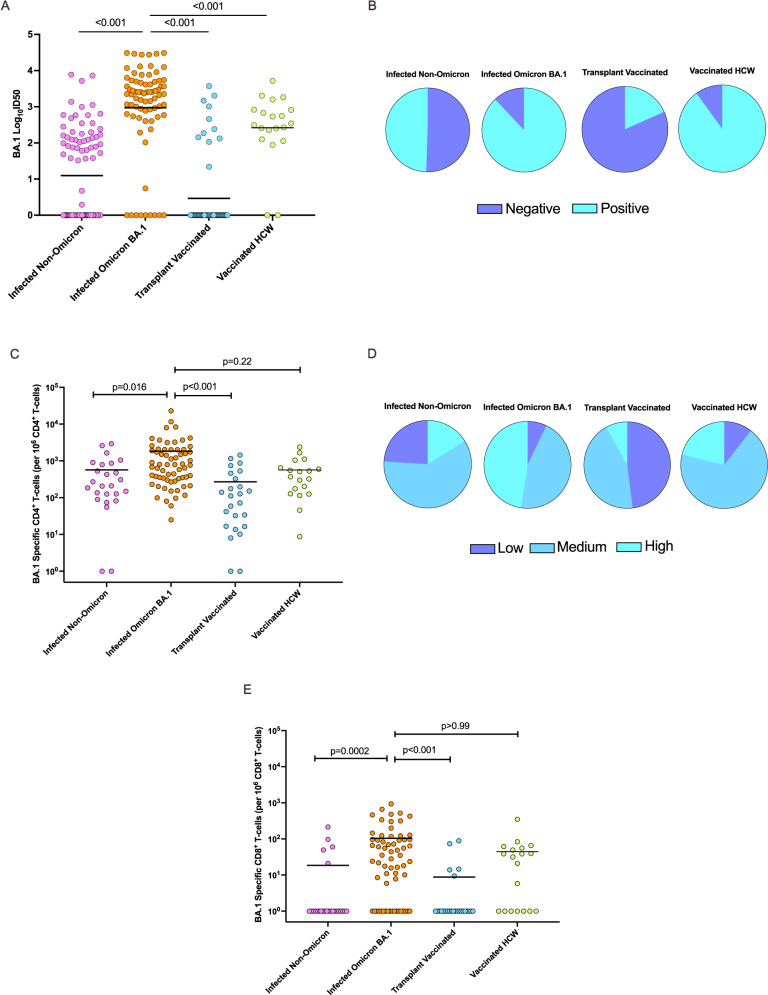
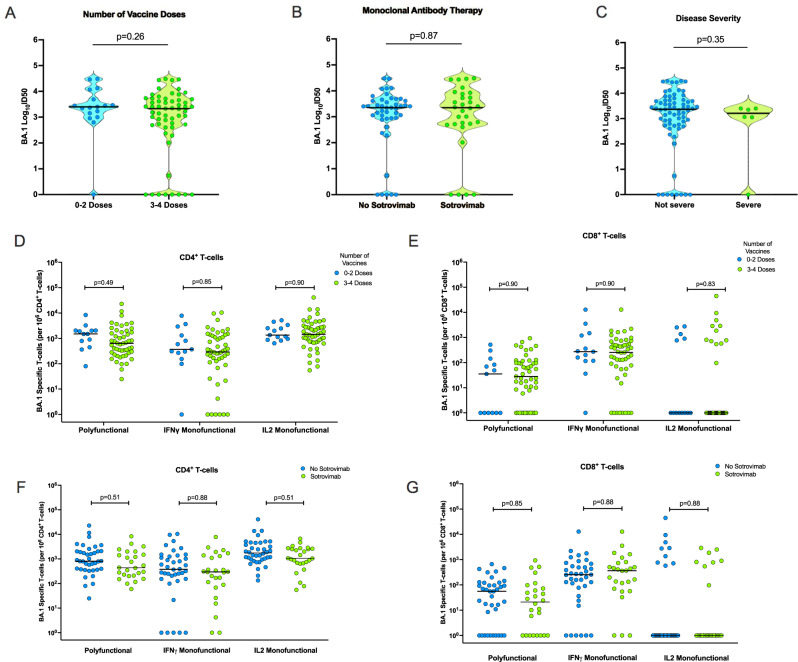
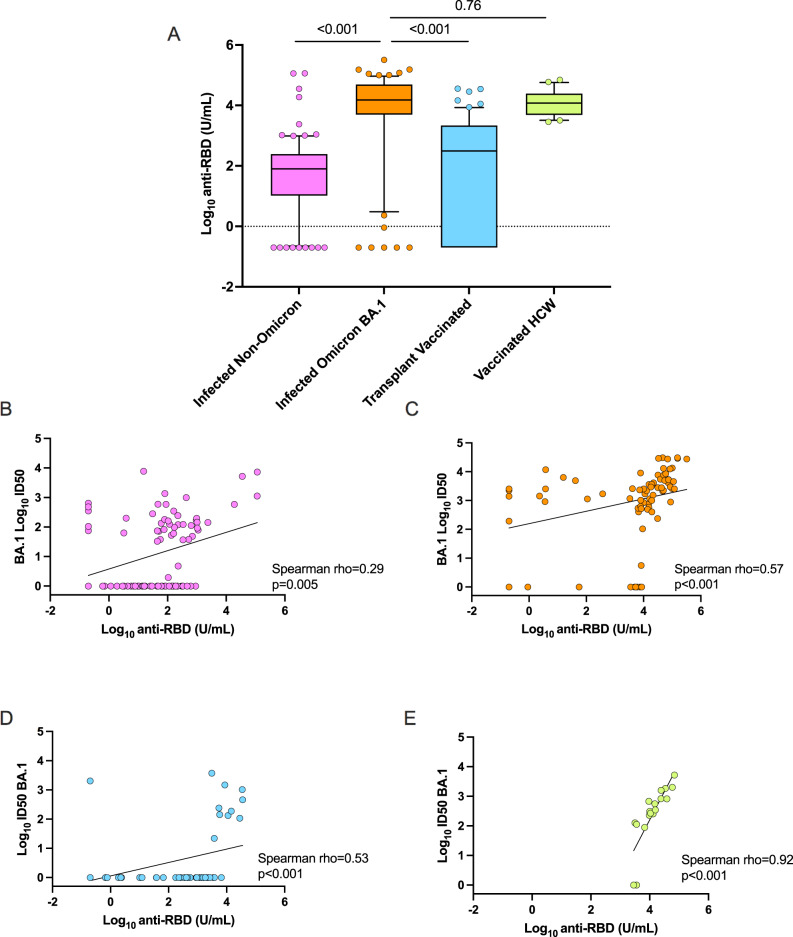
Immunocompromised patients are predisposed to severe COVID-19. Here we compare homotypic and heterotypic humoral and cellular immune responses to Omicron BA.1 in organ transplant patients across a diverse clinical spectrum. We perform variant-specific pseudovirus neutralization assays for D614G, and Omicron-BA.1, -BA.2, and Delta variants. We also measure poly-and monofunctional T-cell responses to BA.1 and ancestral SARS-CoV-2 peptide pools. We identify that partially or fully-vaccinated transplant recipients after infection with Omicron BA.1 have the greatest BA.1 neutralizing antibody and BA.1-specific polyfunctional CD4+ and CD8+ T-cell responses, with potent cross-neutralization against BA.2. In these patients, the magnitude of the BA.1-directed response is comparable to immunocompetent triple-vaccinated controls. A subset of patients with pre-Omicron infection have heterotypic responses to BA.1 and BA.2, whereas uninfected transplant patients with three doses of vaccine demonstrate the weakest comparative responses. These results have implications for risk of infection, re-infection, and disease severity among immune compromised hosts with Omicron infection.
© 2022. The Author(s).
Conflict of interest statement
D.K. has received research grant from Roche, GSK, and advisory fees from Roche, GSK, Sanofi, Merck and Exevir. A.H. has received research grants from Roche and Merck and advisory fees from Merck and Takeda. A.C.G. has received research funds from a research contract with Providence Therapeutics Holdings, Inc for other projects. No other authors have competing interests to disclose.
Figures
Similar articles
-
Immune responses in COVID-19 patients during breakthrough infection with SARS-CoV-2 variants Delta, Omicron-BA.1 and Omicron-BA.5.Front Immunol. 2023 Jul 13;14:1150667. doi: 10.3389/fimmu.2023.1150667. eCollection 2023. Front Immunol. 2023. PMID: 37520539 Free PMC article.
-
Neutralization sensitivity, fusogenicity, and infectivity of Omicron subvariants.Genome Med. 2022 Dec 29;14(1):146. doi: 10.1186/s13073-022-01151-6. Genome Med. 2022. PMID: 36581867 Free PMC article.
-
Omicron BA.4/5 Neutralization and T-Cell Responses in Organ Transplant Recipients After Booster Messenger RNA Vaccine: A Multicenter Cohort Study.Clin Infect Dis. 2023 Jul 26;77(2):229-236. doi: 10.1093/cid/ciad175. Clin Infect Dis. 2023. PMID: 36975097
-
Dynamics of viral shedding during ancestral or Omicron BA.1 SARS-CoV-2 infection and enhancement of pre-existing immunity during breakthrough infections.Emerg Microbes Infect. 2022 Dec;11(1):2423-2432. doi: 10.1080/22221751.2022.2122578. Emerg Microbes Infect. 2022. PMID: 36098494 Free PMC article.
-
Monoclonal antibodies as COVID-19 prophylaxis therapy in immunocompromised patient populations.Int J Infect Dis. 2023 Sep;134:228-238. doi: 10.1016/j.ijid.2023.06.021. Epub 2023 Jul 1. Int J Infect Dis. 2023. PMID: 37400053 Review.
Cited by
-
Heterologous versus homologous boosting elicits qualitatively distinct, BA.5-cross-reactive T cells in transplant recipients.JCI Insight. 2023 May 22;8(10):e168470. doi: 10.1172/jci.insight.168470. JCI Insight. 2023. PMID: 37104041 Free PMC article.
-
Clinical and prognostic implications of hyaluronic acid in patients with COVID-19 reinfection and first infection.Front Microbiol. 2024 May 31;15:1406581. doi: 10.3389/fmicb.2024.1406581. eCollection 2024. Front Microbiol. 2024. PMID: 38881657 Free PMC article.
-
Additive effects of booster mRNA vaccination and SARS-CoV-2 Omicron infection on T cell immunity across immunocompromised states.Sci Transl Med. 2023 Jul 12;15(704):eadg9452. doi: 10.1126/scitranslmed.adg9452. Epub 2023 Jul 12. Sci Transl Med. 2023. PMID: 37437015 Free PMC article.
-
Persistent SARS-CoV-2-specific immune defects in kidney transplant recipients following third mRNA vaccine dose.Am J Transplant. 2023 Jun;23(6):744-758. doi: 10.1016/j.ajt.2023.03.014. Epub 2023 Mar 24. Am J Transplant. 2023. PMID: 36966905 Free PMC article.
-
Precision Vaccinology Approaches for the Development of Adjuvanted Vaccines Targeted to Distinct Vulnerable Populations.Pharmaceutics. 2023 Jun 19;15(6):1766. doi: 10.3390/pharmaceutics15061766. Pharmaceutics. 2023. PMID: 37376214 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
