

Predicting liver regeneration following major resection
- PMID: 35927556
- PMCID: PMC9352754
- DOI: 10.1038/s41598-022-16968-9
Predicting liver regeneration following major resection
Abstract
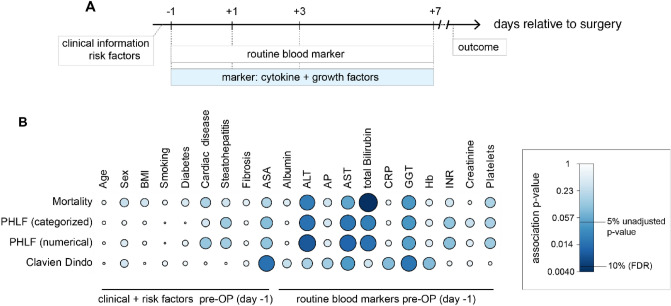
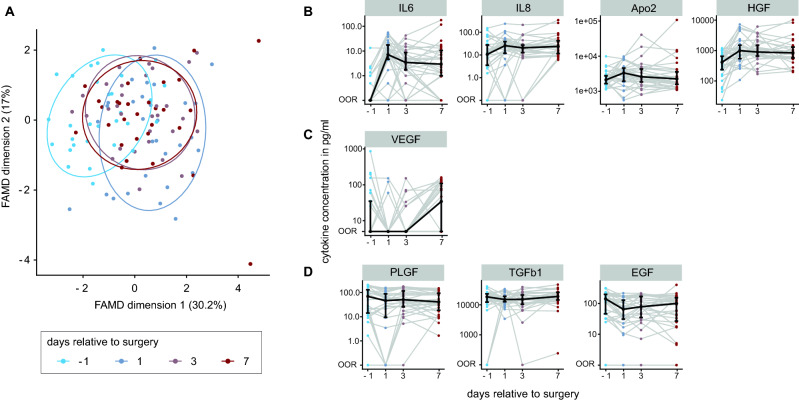
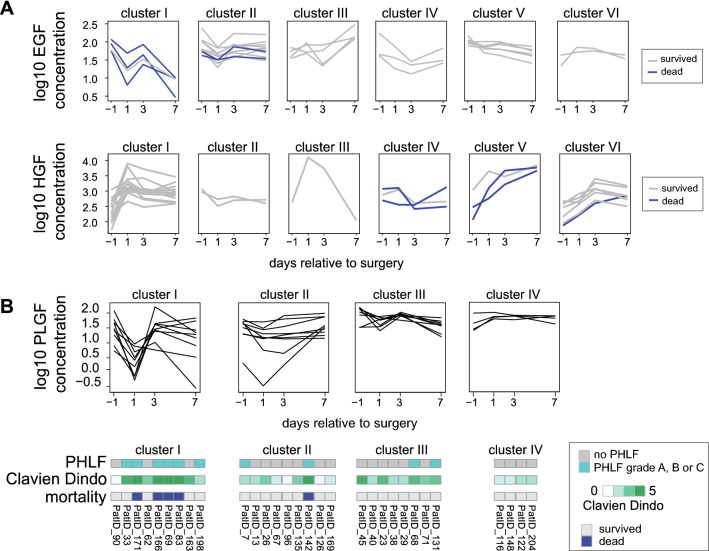
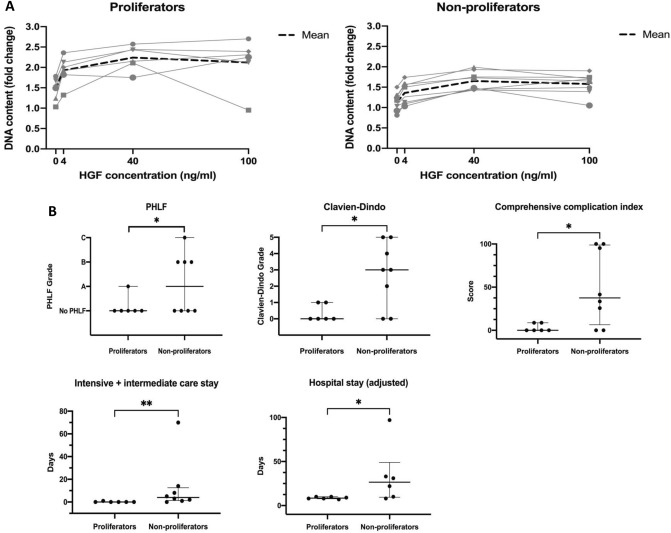
Breakdown of synthesis, excretion and detoxification defines liver failure. Post-hepatectomy liver failure (PHLF) is specific for liver resection and a rightfully feared complication due to high lethality and limited therapeutic success. Individual cytokine and growth factor profiles may represent potent predictive markers for recovery of liver function. We aimed to investigate these profiles in post-hepatectomy regeneration. This study combined a time-dependent cytokine and growth factor profiling dataset of a training (30 patients) and a validation (14 patients) cohorts undergoing major liver resection with statistical and predictive models identifying individual pathway signatures. 2319 associations were tested. Primary hepatocytes isolated from patient tissue samples were stimulated and their proliferation was analysed through DNA content assay. Common expression trajectories of cytokines and growth factors with strong correlation to PHLF, morbidity and mortality were identified despite highly individual perioperative dynamics. Especially, dynamics of EGF, HGF, and PLGF were associated with mortality. PLGF was additionally associated with PHLF and complications. A global association-network was calculated and validated to investigate interdependence of cytokines and growth factors with clinical attributes. Preoperative cytokine and growth factor signatures were identified allowing prediction of mortality following major liver resection by regression modelling. Proliferation analysis of corresponding primary human hepatocytes showed associations of individual regenerative potential with clinical outcome. Prediction of PHLF was possible on as early as first postoperative day (POD1) with AUC above 0.75. Prediction of PHLF and mortality is possible on POD1 with liquid-biopsy based risk profiling. Further utilization of these models would allow tailoring of interventional strategies according to individual profiles.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
