

Functional connectivity in reward circuitry and symptoms of anhedonia as therapeutic targets in depression with high inflammation: evidence from a dopamine challenge study
- PMID: 35927580
- PMCID: PMC9718669
- DOI: 10.1038/s41380-022-01715-3
Functional connectivity in reward circuitry and symptoms of anhedonia as therapeutic targets in depression with high inflammation: evidence from a dopamine challenge study
Erratum in
-
Correction to: Functional connectivity in reward circuitry and symptoms of anhedonia as therapeutic targets in depression with high inflammation: evidence from a dopamine challenge study.Mol Psychiatry. 2022 Oct;27(10):4122. doi: 10.1038/s41380-022-01754-w. Mol Psychiatry. 2022. PMID: 36065017 Free PMC article. No abstract available.
Abstract
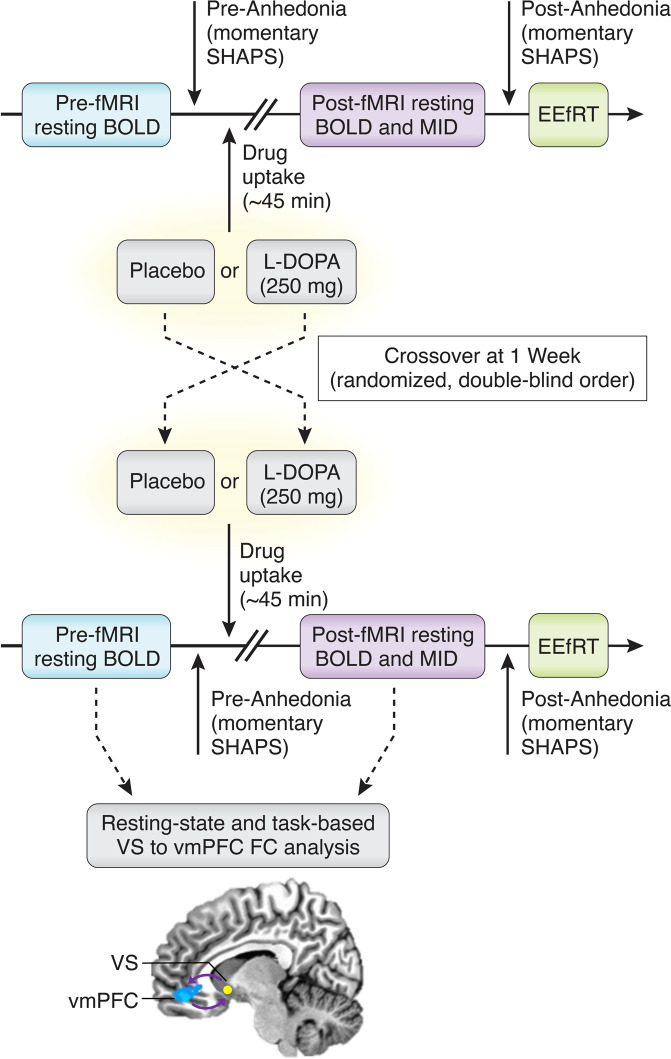
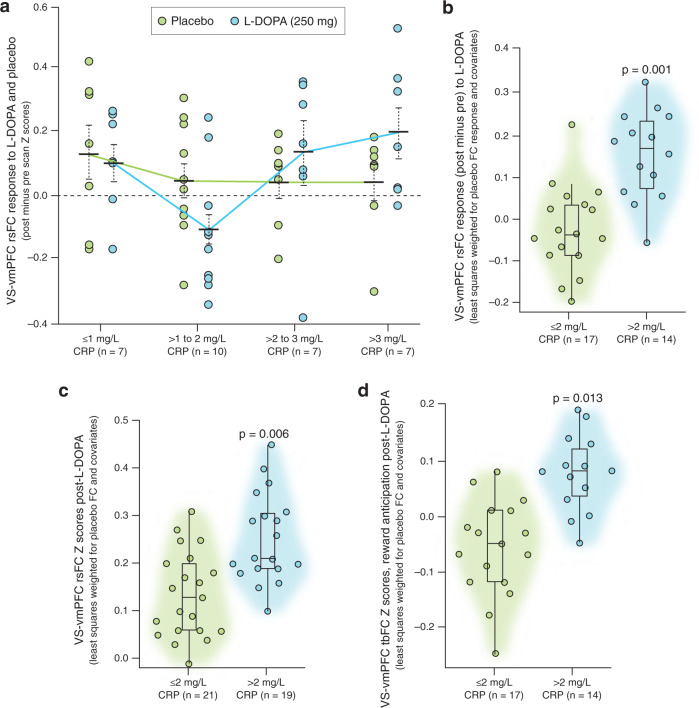
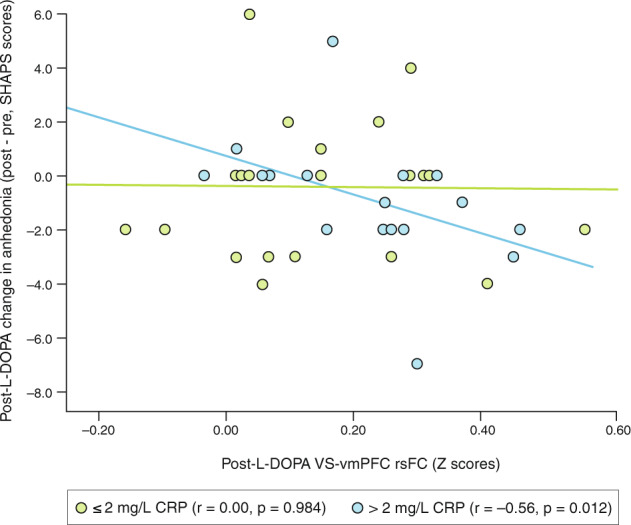
Increased inflammation in major depressive disorder (MDD) has been associated with low functional connectivity (FC) in corticostriatal reward circuits and symptoms of anhedonia, relationships which may involve the impact of inflammation on synthesis and release of dopamine. To test this hypothesis while establishing a platform to examine target engagement of potential therapies in patients with increased inflammation, medically stable unmedicated adult MDD outpatients enrolled to have a range of inflammation (as indexed by plasma C-reactive protein [CRP] levels) were studied at two visits involving acute challenge with the dopamine precursor levodopa (L-DOPA; 250 mg) and placebo (double-blind, randomized order ~1-week apart). The primary outcome of resting-state (rs)FC in a classic ventral striatum to ventromedial prefrontal cortex reward circuit was calculated using a targeted, a priori approach. Data available both pre- and post-challenge (n = 31/40) established stability of rsFC across visits and determined CRP > 2 mg/L as a cut-point for patients exhibiting positive FC responses (post minus pre) to L-DOPA versus placebo (p < 0.01). Higher post-L-DOPA FC in patients with CRP > 2 mg/L was confirmed in all patients (n = 40) where rsFC data were available post-challenge (B = 0.15, p = 0.006), and in those with task-based (tb)FC during reward anticipation (B = 0.15, p = 0.013). While effort-based motivation outside the scanner positively correlated with rsFC independent of treatment or CRP, change in anhedonia scores negatively correlated with rsFC after L-DOPA only in patients with CRP > 2 mg/L (r = -0.56, p = 0.012). FC in reward circuitry should be further validated in larger samples as a biomarker of target engagement for potential treatments including dopaminergic agents in MDD patients with increased inflammation.
© 2022. The Authors.
Conflict of interest statement
In the past 3 years, JCF has consulted for Otsuka and Health BioConsulting on topics unrelated to this work. MTT has served as a paid consultant to Blackthorn Therapeutics. MTT is a co-inventor of the EEfRT, which is discussed in this manuscript. Emory University and Vanderbilt University licensed this software to BlackThorn Therapeutics. Under the IP Policies of both universities, MTT receives licensing fees and royalties from BlackThorn Therapeutics. Additionally, MTT has a paid consulting relationship with BlackThorn. The terms of these arrangements have been reviewed and approved by Emory University in accordance with its conflict-of-interest policies, and no funding from these entities was used to support the current work. The remaining authors declare no competing interests. All views expressed are solely those of the authors.
Figures
References
-
- Swardfager W, Rosenblat JD, Benlamri M, McIntyre RS. Mapping inflammation onto mood: inflammatory mediators of anhedonia. Neurosci Biobehav Rev. 2016;64:148–66. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
