

What next for the polyclinic? New models of primary health care are required in many former Soviet Union countries
- PMID: 35927680
- PMCID: PMC9354434
- DOI: 10.1186/s12875-022-01812-w
What next for the polyclinic? New models of primary health care are required in many former Soviet Union countries
Abstract
Background: There is unfinished reform in primary care in Russia and other former Soviet Union (FSU) countries. The traditional 'Semashko' multi-specialty polyclinic model has been retained, while its major characteristics are increasingly questioned. The search for a new model is on a health policy agenda. It is relevant for many other countries.
Objectives: In this paper, we explore the strengths and weaknesses of the multi-specialty polyclinic model currently found in Russia and other FSU countries, as well as the features of the emerging multi-disciplinary and large-scale primary care models internationally. The comparison of the two is a major research question. Health policy implications are discussed.
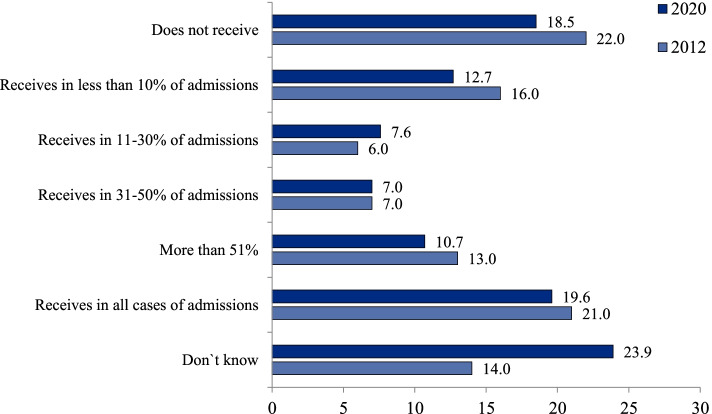
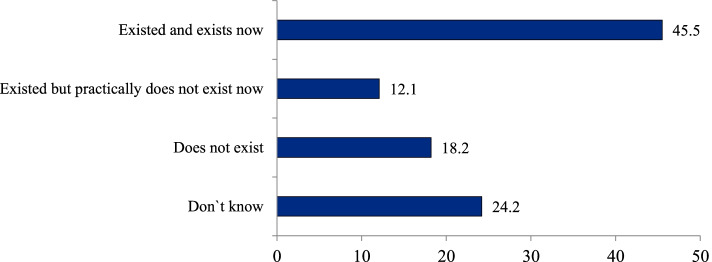
Methods: We use data from two physicians' surveys and recent literature to identify the characteristics of multi-specialty polyclinics, indicators of their performance and the evaluation in the specific country context. The review of the literature is used to describe new primary care models internationally.
Results: The Semashko polyclinic model has lost some of its original strengths due to the excessive specialization of service delivery. We demonstrate the strengths of extended practices in Western countries and conclude that FSU countries should "leapfrog" the phase of developing solo practices and build a multi-disciplinary model similar to the extended practices model in Europe. The latter may act as a 'golden mean' between the administrative dominance of the polyclinic model and the limited capacity of solo practices. The new model requires a separation of primary care and outpatient specialty care, with the transformation of polyclinics into centers of outpatient diagnostic and specialty services that become part of hospital services while working closely with primary care.
Conclusion: The comprehensiveness of care in a big setting and potential economies of scale, which are major strengths of the polyclinic model, should be retained in the provision of specialty care rather than primary care. Internationally, there are lessons about the risks associated with models based on narrow specialization in caring for patients who increasingly have multiple conditions.
Keywords: Multi-specialty model; Polyclinic; Primary health care.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Kuhlbrandt C. Primary care reforms in countries of the former Soviet Union: success and challenges. In: Rechel B, Richardson E, McKee M, editors. Trends in health systems in the former Soviet countries. Copenhagen: World Health Organization; 2014.
-
- Kringos D, Boerma W, Hutchinson A, Saltman R. Building primary care in a changing Europe. Vol. 1, No. 38. Copenhagen: The European Observatory on Health Systems and Health Policies; 2015. - PubMed
-
- Jakab M, Farrington J, Borgermans L, Mantingh F. Health systems respond to noncommunicable diseases: time for ambition. Copenhagen: WHO Regional Office for Europe; 2018. p. 137.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources