

Cardiovascular outcomes trials: a paradigm shift in the current management of type 2 diabetes
- PMID: 35927730
- PMCID: PMC9351217
- DOI: 10.1186/s12933-022-01575-9
Cardiovascular outcomes trials: a paradigm shift in the current management of type 2 diabetes
Abstract
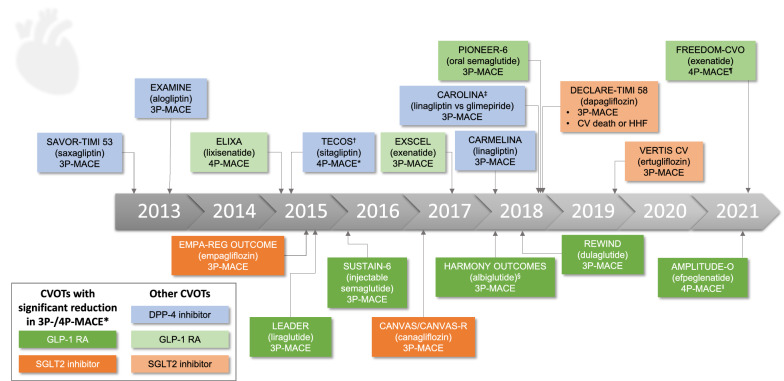
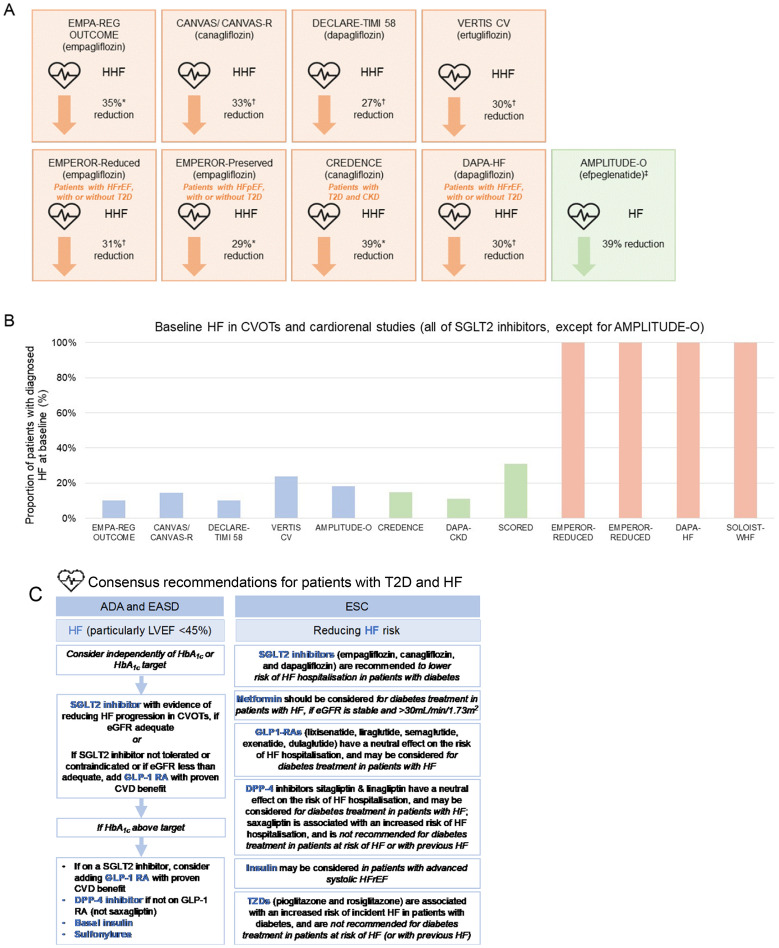
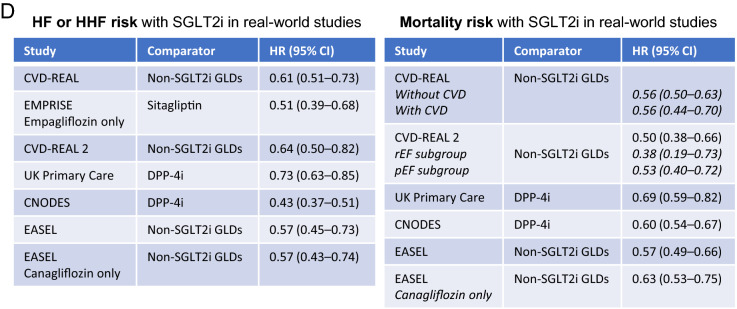
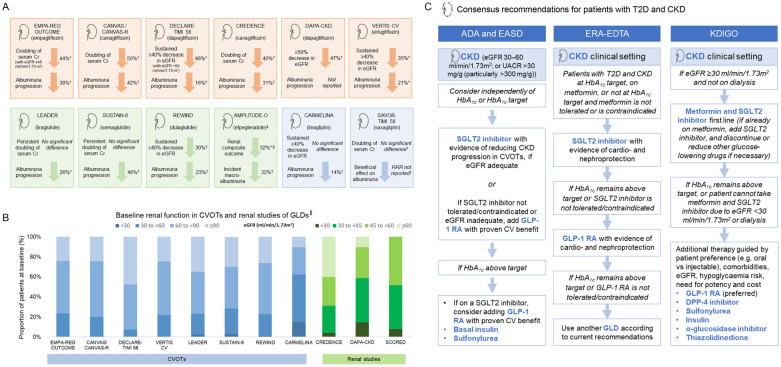
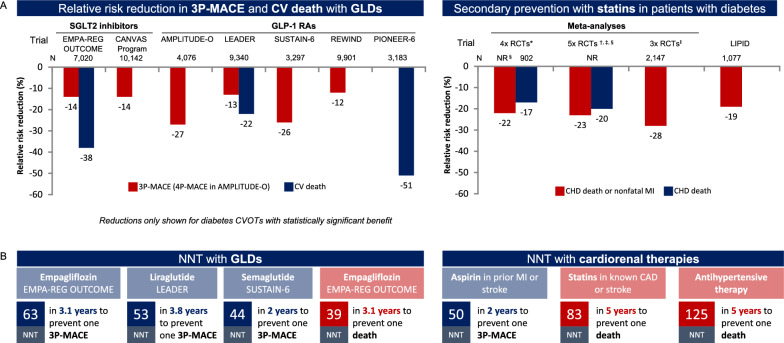
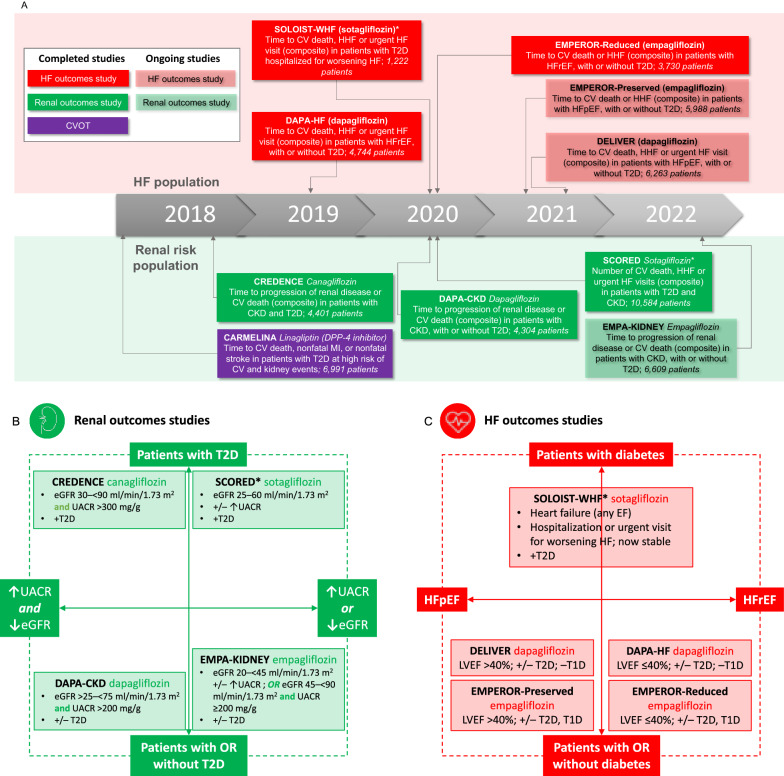
Cardiovascular disease (CVD) is the leading cause of mortality and morbidity in patients with type 2 diabetes (T2D). Historical concerns about cardiovascular (CV) risks associated with certain glucose-lowering medications gave rise to the introduction of cardiovascular outcomes trials (CVOTs). Initially implemented to help monitor the CV safety of glucose-lowering drugs in patients with T2D, who either had established CVD or were at high risk of CVD, data that emerged from some of these trials started to show benefits. Alongside the anticipated CV safety of many of these agents, evidence for certain sodium-glucose transporter 2 (SGLT2) inhibitors and glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have revealed potential cardioprotective effects in patients with T2D who are at high risk of CVD events. Reductions in 3-point major adverse CV events (3P-MACE) and CV death have been noted in some of these CVOTs, with additional benefits including reduced risks of hospitalisation for heart failure, progression of renal disease, and all-cause mortality. These new data are leading to a paradigm shift in the current management of T2D, with international guidelines now prioritising SGLT2 inhibitors and/or GLP-1 RAs in certain patient populations. However, clinicians are faced with a large volume of CVOT data when seeking to use this evidence base to bring opportunities to improve CV, heart failure and renal outcomes, and even reduce mortality, in their patients with T2D. The aim of this review is to provide an in-depth summary of CVOT data-crystallising the key findings, from safety to efficacy-and to offer a practical perspective for physicians. Finally, we discuss the next steps for the post-CVOT era, with ongoing studies that may further transform clinical practice and improve outcomes for people with T2D, heart failure or renal disease.
Keywords: CVOTs; Cardiovascular disease; Cardiovascular outcomes trials; Cardiovascular safety; Chronic kidney disease; GLP-1 RAs; Glucose-lowering drug; Heart failure; SGLT2 inhibitors; Type 2 diabetes.
© 2022. The Author(s).
Conflict of interest statement
MJD reported board membership and consultancy fees from Novo Nordisk, Sanofi-Aventis, Lilly, Merck, Sharp & Dohme, Boehringer Ingelheim, AstraZeneca, Servier, and Janssen. MJD reported institutional grants from Novo Nordisk, Sanofi-Aventis, Lilly, Boehringer Ingelheim and Janssen. MJD reported payment for lectures or speaker bureaus from Novo Nordisk, Sanofi-Aventis, Lilly, Merck, Sharp & Dohme, Boehringer Ingelheim, AstraZeneca, Janssen, Mitsubishi Tanabe Pharma, and Takeda Pharmaceuticals International.
HD declares no conflicts of interest.
FRJ has received consulting honoraria from Boehringer Ingelheim, Mundipharma, Astra Zeneca, Novo Nordisk, MSD, Lilly, and Sanofi.DKM has had leadership roles in clinical trials for AstraZeneca, Boehringer Ingelheim, Eisai, Esperion, GlaxoSmithKline, Janssen, Lexicon, Merck & Co., Inc., Novo Nordisk, CSL Behring, and Sanofi USA; and has received consultancy fees from AstraZeneca, Boehringer Ingelheim, Lilly USA, Merck & Co., Inc., Pfizer, Novo Nordisk, Metavant, Afimmune, and Sanofi.
ZP has received consulting honoraria from Boehringer Ingelheim, Novo Nordisk, and Sanofi.
PMS has received honorarium for lectures for Medtronic, Abbott, Servier, Astra Zeneca, and Respicardia; Boehringer Ingelheim consultancy agreement and honorarium for lecture, Novartis consultancy agreement and honorarium for lecture, Vifor Pharma consultancy agreement.
CW has received personal fees from Boehringer Ingelheim, Akebia, AstraZeneca, Bayer, Eli Lilly, GlaxoSmithKline, Gilead, Merck Sharpe Dohme, Mundipharma, Sanofi-Genzyme, and Vifor Fresenius.
Figures

References
-
- Nwaneri C, Cooper H, Bowen-Jones D. Mortality in type 2 diabetes mellitus: magnitude of the evidence from a systematic review and meta-analysis. Br J Diabetes Vasc Dis. 2013;13:192–207. doi: 10.1177/1474651413495703. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
