

Time to reconcile research findings and clinical practice on upper limb neurorehabilitation
- PMID: 35928130
- PMCID: PMC9343948
- DOI: 10.3389/fneur.2022.939748
Time to reconcile research findings and clinical practice on upper limb neurorehabilitation
Abstract
The problem: In the field of upper limb neurorehabilitation, the translation from research findings to clinical practice remains troublesome. Patients are not receiving treatments based on the best available evidence. There are certainly multiple reasons to account for this issue, including the power of habit over innovation, subjective beliefs over objective results. We need to take a step forward, by looking at most important results from randomized controlled trials, and then identify key active ingredients that determined the success of interventions. On the other hand, we need to recognize those specific categories of patients having the greatest benefit from each intervention, and why. The aim is to reach the ability to design a neurorehabilitation program based on motor learning principles with established clinical efficacy and tailored for specific patient's needs.
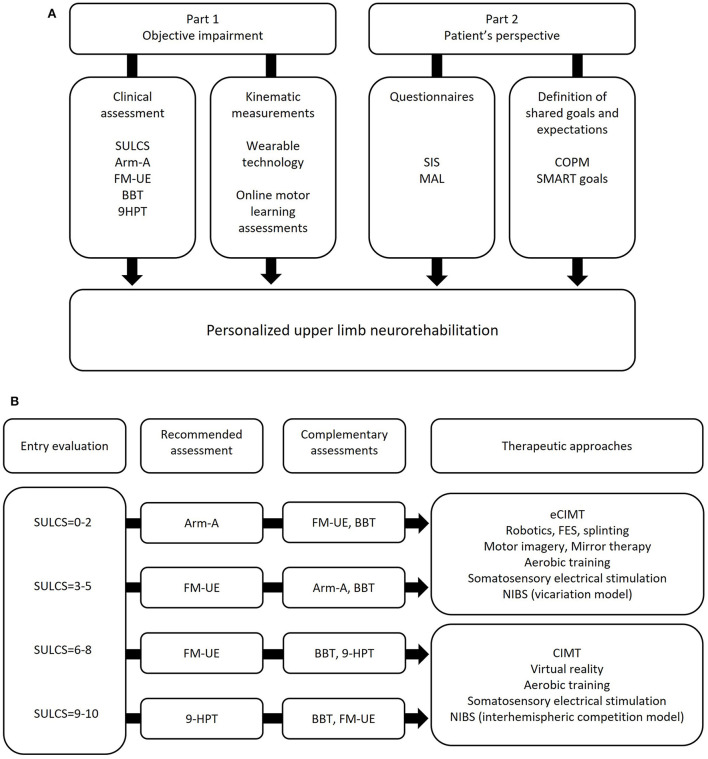
Proposed solutions: The objective of the present manuscript is to facilitate the translation of research findings to clinical practice. Starting from a literature review of selected neurorehabilitation approaches, for each intervention the following elements were highlighted: definition of active ingredients; identification of underlying motor learning principles and neural mechanisms of recovery; inferences from research findings; and recommendations for clinical practice. Furthermore, we included a dedicated chapter on the importance of a comprehensive assessment (objective impairments and patient's perspective) to design personalized and effective neurorehabilitation interventions.
Conclusions: It's time to reconcile research findings with clinical practice. Evidence from literature is consistently showing that neurological patients improve upper limb function, when core strategies based on motor learning principles are applied. To this end, practical take-home messages in the concluding section are provided, focusing on the importance of graded task practice, high number of repetitions, interventions tailored to patient's goals and expectations, solutions to increase and distribute therapy beyond the formal patient-therapist session, and how to integrate different interventions to maximize upper limb motor outcomes. We hope that this manuscript will serve as starting point to fill the gap between theory and practice in upper limb neurorehabilitation, and as a practical tool to leverage the positive impact of clinicians on patients' recovery.
Keywords: motor learning; neurorehabilitation; personalized medicine; stroke; upper limb.
Copyright © 2022 Boccuni, Marinelli, Trompetto, Pascual-Leone and Tormos Muñoz.
Figures
Similar articles
-
Construction of efficacious gait and upper limb functional interventions based on brain plasticity evidence and model-based measures for stroke patients.ScientificWorldJournal. 2007 Dec 20;7:2031-45. doi: 10.1100/tsw.2007.299. ScientificWorldJournal. 2007. PMID: 18167618 Free PMC article.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
The Effectiveness of Integrated Care Pathways for Adults and Children in Health Care Settings: A Systematic Review.JBI Libr Syst Rev. 2009;7(3):80-129. doi: 10.11124/01938924-200907030-00001. JBI Libr Syst Rev. 2009. PMID: 27820426
-
Principles of Neurorehabilitation After Stroke Based on Motor Learning and Brain Plasticity Mechanisms.Front Syst Neurosci. 2019 Dec 17;13:74. doi: 10.3389/fnsys.2019.00074. eCollection 2019. Front Syst Neurosci. 2019. PMID: 31920570 Free PMC article. Review.
-
Neurotechnology-aided interventions for upper limb motor rehabilitation in severe chronic stroke.Brain. 2019 Aug 1;142(8):2182-2197. doi: 10.1093/brain/awz181. Brain. 2019. PMID: 31257411 Free PMC article. Review.
Cited by
-
Implementing modified constraint-induced movement therapy after stroke in an early-supported discharge rehabilitation service: a process evaluation using RE-AIM QuEST.BMC Health Serv Res. 2025 Aug 15;25(1):1086. doi: 10.1186/s12913-025-13273-9. BMC Health Serv Res. 2025. PMID: 40817048 Free PMC article.
-
Flexibility, Resistance, Aerobic, Movement Execution (FRAME) training program to improve gait capacity in adults with Hereditary Spastic Paraplegia: protocol for a single-cohort feasibility trial.Front Neurol. 2025 Feb 18;16:1441512. doi: 10.3389/fneur.2025.1441512. eCollection 2025. Front Neurol. 2025. PMID: 40040914 Free PMC article.
-
Role of Yoga as Adjunctive Therapy for Migraines: A Narrative Review of the Literature.Cureus. 2023 Nov 7;15(11):e48434. doi: 10.7759/cureus.48434. eCollection 2023 Nov. Cureus. 2023. PMID: 38073999 Free PMC article. Review.
-
Neurorehabilitation of the upper extremity - immersive virtual reality vs. electromechanically assisted training. A comparative study.Front Neurol. 2023 Dec 21;14:1290637. doi: 10.3389/fneur.2023.1290637. eCollection 2023. Front Neurol. 2023. PMID: 38187150 Free PMC article.
-
Padua Days on Muscle and Mobility Medicine, March 25-29, 2025, Hotel Petrarca, Euganean Thermae, Italy: Program and Abstracts.Eur J Transl Myol. 2025 Mar 31;35(1):13789. doi: 10.4081/ejtm.2025.13789. Epub 2025 Mar 5. Eur J Transl Myol. 2025. PMID: 40047227 Free PMC article.
References
-
- Morris DM, Taub E, Mark VW. Constraint-induced movement therapy: characterizing the intervention protocol. Eur Medicophysica. (2006) 42:257–68. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous